Osteoarthritis (OA) is more than just wear-and-tear on your joints; it’s a common degenerative condition that affects millions of people worldwide.
In OA, the protective cartilage that cushions your joints gradually breaks down, causing bones to rub together. This can lead to discomfort, reduced flexibility, and challenges in performing everyday activities.
The knees, hips, hands, spine, and other weight-bearing joints are most often affected.
Because it develops slowly, many people try to adapt to mild symptoms. Without proper care, osteoarthritis can progress, limiting mobility and overall quality of life.
In this post, we’ll explore what osteoarthritis is, its causes, symptoms, treatments, and ways you can prevent or manage it to keep your joints healthy and active.
What is Osteoarthritis?
Osteoarthritis is the most common form of arthritis, a condition that affects the joints. It develops when the cartilage that cushions your joints gradually wears down, causing the bones to rub against each other during movement.
OA affects the entire joint (bones, cartilage, ligaments, and synovium) and can also cause bone spurs (osteophytes) to form at the edges.
Because of these changes, OA is often called a degenerative arthritis or degenerative joint disease.
Osteoarthritis can affect any joint in the body, but it most commonly occurs in the:
- Hands
- Knees
- Hips
- Neck (cervical spine)
- Lower back (lumbar spine)
Symptoms usually develop gradually and may worsen over time, especially with regular joint use.
What are the Types of Osteoarthritis?
Osteoarthritis is generally classified into two main types based on its cause: primary osteoarthritis and secondary osteoarthritis.
Primary Osteoarthritis
Primary osteoarthritis is the most common form of OA. It develops slowly over time, usually as a result of aging and long-term joint use.
Rather than having one clear cause, it is linked to multiple risk factors such as increasing age, genetic predisposition, obesity, and everyday wear and tear on the joints.
Secondary Osteoarthritis
Secondary osteoarthritis occurs when joint damage is triggered by a specific condition or injury.
This may include a past joint injury, repetitive stress from sports or physical work, joint deformities present at birth, or other joint diseases such as rheumatoid arthritis.
In these cases, identifying and managing the underlying cause can help slow the progression of osteoarthritis.

What are the Causes of Osteoarthritis?
Osteoarthritis results from the gradual breakdown of joint cartilage and changes to nearby bone structures. Several risk factors are known to increase the risk of developing osteoarthritis:
- Age: OA is more common as people get older. The cartilage repair process slows with age, so even normal daily stress can lead to damage.
- Genetics: Family history of OA raises risk. Genetic factors may influence cartilage strength and bone shape.
- Gender: Women, especially after menopause, are more likely to develop OA than men.
- Obesity: Excess body weight adds stress to weight-bearing joints (knees, hips, spine) and may produce inflammatory chemicals.
- Joint Injuries/Overuse: Past injuries (fractures, torn ligaments, or meniscus) or repeated stress from sports and certain jobs can precipitate OA.
- Falls: Falls can injure joints or bones, leading to long-term joint damage that may later develop into osteoarthritis.
- Mechanical/Structural Issues: Abnormal joint anatomy (like bowed legs or hip dysplasia) or weak muscles around a joint can increase wear and tear.
- Metabolic and Medical Conditions: Some diseases (e.g., diabetes, hemochromatosis) and certain forms of inflammatory arthritis (e.g., gout) can damage cartilage, leading to secondary OA.
- Certain Health Conditions: Disorders such as Ehlers-Danlos syndrome or joint hypermobility syndrome weaken joint support and make joints more prone to osteoarthritis over time.

What are the Signs and Symptoms of Osteoarthritis?
Symptoms of osteoarthritis often start gradually and typically affect one or a few joints. Common symptoms include:
- Joint Pain and Aching: A deep, throbbing pain in the joint that worsens with use (walking, climbing stairs, etc.) and often improves with rest.
- Stiffness: Joints feel stiff, particularly after inactivity. Morning stiffness lasting less than ~30 minutes is classic for OA.
- Tenderness or Swelling: The joint may be tender to the touch and sometimes swollen. Inactivity or overuse can trigger mild swelling or warmth around the joint.
- Limited Flexibility: Range of motion decreases as cartilage thins. Over time, you may lose some ability to straighten or bend the joint fully.
- Crepitus (Grating or Crackling): You may feel or hear a grating, crackling, or popping sensation when moving the joint. This comes from rough cartilage surfaces and bone rubbing.
- Bone Spurs (Osteophytes): Hard bony lumps can form at the joint edges. These may be felt as bumps (e.g., on finger joints) and contribute to pain and reduced range of motion.
- Weakness or Instability: Muscle weakness around the joint can make it feel like it will give way (especially the knee). In severe OA, misalignment or deformity of the joint may develop.
These symptoms usually build over time. A person may first notice occasional discomfort or slight stiffness after activity, which gradually worsens.
In advanced OA, the joint may ache even at rest, and daily activities become limited.

How to Treat Osteoarthritis?
Your healthcare provider will help create a treatment plan to manage your osteoarthritis symptoms and improve joint function.
While there is no cure for osteoarthritis, and damaged cartilage cannot be restored, many treatments can reduce pain, ease stiffness, and help you stay active.
Common treatments for osteoarthritis include:
Lifestyle Management
Lifestyle changes are the foundation of OA treatment. For example:
- Weight Management: Losing body weight can dramatically reduce pain and improve function in knee and hip OA.
- Exercise: Low-impact aerobic exercise (walking, cycling, swimming) improves cardiovascular health and endurance.
- Activity Pacing & Joint Protection: Learning to balance activity with rest, using assistive devices (cane, jar opener), and modifying tasks to reduce joint strain.
- Healthy Diet: An anti-inflammatory diet rich in fruits, vegetables, whole grains, and omega-3 fatty acids (fish) may help.
Physical and Complementary Therapies
Physical therapy and related therapies are key to managing OA. Most common ones include:
- Physical Therapy (PT): A PT can design a customized exercise program, teach proper body mechanics, and use modalities like ultrasound or TENS (transcutaneous electrical nerve stimulation) for pain relief.
- Heat and cold therapy: Applying heat or cold to painful joints may relieve discomfort and stiffness.
- Occupational Therapy (OT): OTs help adapt the home and workplace and recommend assistive devices to maintain independence.
- Acupuncture: Some patients find significant pain relief, which is thought to stimulate the release of natural pain-relieving chemicals.
- Bracing & Orthotics: Knee braces can provide stability and unload specific knee compartments. Shoe inserts (orthotics) can help with alignment and reduce stress on knees and hips.
Medications
Some medications are used to control pain and inflammation, but always under medical guidance.
- Topical Analgesics: Creams, gels, or patches containing NSAIDs (diclofenac) or capsaicin can provide localized pain relief with minimal systemic side effects.
- Oral Pain Relievers:
- Acetaminophen: First-line for mild to moderate pain, but has limits on daily dosage.
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): Effective for pain and inflammation but carry risks of stomach, heart, and kidney issues with long-term use.
- Duloxetine: An antidepressant that is FDA-approved for chronic musculoskeletal pain, including OA.
- Supplements: Glucosamine and chondroitin sulfate may provide modest symptom relief for some, though evidence is mixed. They are generally safe.
Injections
For when oral medications and therapy are insufficient, a healthcare professional might recommend injections, such as:
- Corticosteroid Injections: Powerful anti-inflammatory injections that can provide weeks to months of pain relief.
- Hyaluronic Acid (Viscosupplementation) Injections: Injected into the knee, these aim to supplement the joint’s natural lubricating fluid, providing cushioning.
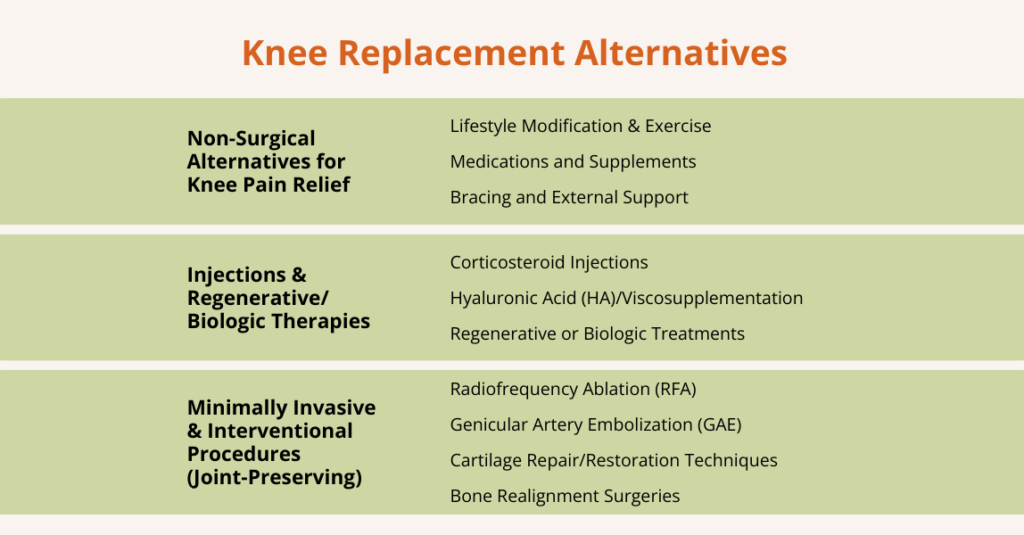
Minimally Invasive Treatments
Minimally invasive treatments are designed to reduce pain and improve joint function without major surgery.
For example, Genicular Artery Embolization (GAE) is a minimally invasive procedure used mainly for knee osteoarthritis. It works by blocking tiny inflamed blood vessels around the knee joint that contribute to pain.
By reducing inflammation, GAE can relieve pain, improve mobility, and help some patients delay or avoid knee replacement surgery. It does not repair damaged cartilage but can provide meaningful symptom relief.
Surgical Interventions
Considered when conservative treatments fail, and quality of life is severely impacted.
- Arthroscopy: Cleans out debris and repairs torn cartilage. Primarily useful for specific mechanical symptoms, not generalized OA.
- Osteotomy: Realigns bone to shift weight away from the damaged part of the joint (common in knee OA for younger, active patients).
- Joint Replacement (Arthroplasty): The gold standard for end-stage, severe OA. Damaged joint surfaces are replaced with metal and plastic components.
How to Prevent Osteoarthritis?
While not all OA can be prevented, several strategies can help reduce risk:
- Maintain a Healthy Weight: This is the most impactful modifiable factor for preventing knee pain and slowing its progression.
- Stay Active with Smart Exercise: Regular, moderate exercise strengthens muscles and nourishes cartilage. Prioritize low-impact activities and include strength training.
- Prevent Injuries: Use proper techniques and protective gear during sports and work. Rehabilitate fully from any joint injury.
- Listen to Your Body: Pay attention to pain. It is a signal to modify activity, not necessarily to stop altogether.
- Manage Blood Sugar: Evidence links diabetes to faster OA progression, likely due to systemic inflammation and advanced glycation end products (AGEs) that stiffen tissues.
- Eat a Joint-Healthy Diet: A balanced diet supports overall health and may help maintain healthy cartilage.
Frequently Asked Questions (FAQs)
What does osteoarthritis feel like?
People with OA typically experience a deep, aching pain in the affected joint that worsens with use. As it progresses, you may experience stiffness when you first get up, a grating sensation when moving, and pain with everyday motions. Swelling and tenderness can make the joint feel full and sensitive to touch.
When does osteoarthritis start?
OA usually develops gradually and is most common in older adults. Symptoms often appear after age 50 and become more prevalent with advancing age. However, cartilage wear can begin earlier, especially if there was a prior joint injury or excessive joint stress. In fact, research shows that many people over age 60 have some OA changes on X-rays, even if they don’t have symptoms. If you have risk factors (like a knee injury, obesity, or family history), OA can start in middle age or even younger.
What is the best treatment for osteoarthritis?
There is no single best treatment; it is a personalized, multi-faceted approach. Non-drug strategies are considered first-line: staying active, doing physical therapy exercises, and losing weight if needed. These lifestyle measures can reduce pain and improve joint function. Over-the-counter pain relievers (NSAIDs, acetaminophen) or topical creams can help control symptoms. For many patients, combining exercise, weight management, and pain medications works better than any single therapy. In more severe cases, doctors may add injections or recommend surgery.
Is osteoarthritis an autoimmune disease?
No. Osteoarthritis is not autoimmune. It is a degenerative (wear-and-tear) arthritis caused by the mechanical breakdown of joint cartilage, not by the immune system attacking the joint.
Conclusion
Osteoarthritis is a common joint condition that can cause pain, stiffness, and reduced mobility, often impacting daily life and overall well-being.
However, understanding the condition is the first step toward managing it effectively.
By noticing early symptoms and being aware of risk factors, such as past injuries, aging, or excess weight, you can take meaningful steps to protect your joints and your daily life.
The good news is that there are many ways to manage osteoarthritis and stay active.
Gentle, low-impact exercise, physical therapy, and maintaining a healthy weight all help keep your joints strong and flexible.
When pain persists, medications, injections, or minimally invasive treatments can provide relief and help you stay mobile.
With the right combination of lifestyle habits, professional guidance, and support, most people with osteoarthritis can continue to live active, fulfilling lives.