Uterine fibroids are a common health concern affecting many women, often during their reproductive years. While some fibroids remain asymptomatic, others can significantly impact daily life through pain, pressure, and heavy menstrual bleeding. For women in Louisiana exploring advanced and less invasive care, understanding available options is essential.
Seamless Medical Centers offers guidance on fibroid treatment in Louisiana with a focus on uterine preservation, highlighting uterine fibroid embolization and other non-surgical approaches. This resource is designed to help women make informed decisions based on symptoms, lifestyle, and long-term health goals.
Understanding Uterine Fibroids
Uterine fibroids are noncancerous growths that develop in or around the uterus. They vary in size, number, and location, and symptoms can differ widely from one person to another.
Common symptoms of fibroids
Heavy or prolonged menstrual bleeding
Pelvic pain or pressure
Frequent urination
Pain during intercourse
Lower back discomfort
In many cases, women seek treatment for heavy bleeding during periods when fibroids begin to interfere with normal routines or cause anemia.
Why Treatment May Be Necessary
Not all fibroids require immediate intervention. However, treatment becomes important when symptoms affect quality of life or reproductive health.
Key reasons to consider treatment
Persistent menorrhagia or heavy bleeding
Rapid fibroid growth
Fertility concerns
Chronic pelvic discomfort
Pressure on surrounding organs
For women researching menorrhagia treatment in Louisiana, identifying the root cause is the first step toward effective care.
Overview of Fibroid Treatment Options in Louisiana
There are multiple approaches to fibroid management, ranging from medication to surgery. The right choice depends on factors such as age, symptoms, fibroid size, and future pregnancy plans.
Comparison of treatment options
Treatment Type
Procedure Type
Recovery Time
Uterus Preserved
Best For
Medication
Non-invasive
Minimal
Yes
Mild symptoms
Myomectomy
Surgical
Moderate
Yes
Fertility preservation
Hysterectomy
Surgical
Longer
No
Severe cases
Uterine Fibroid Embolization
Minimally invasive
Short
Yes
Symptomatic fibroids
For many women seeking fibroid treatment without surgery in Louisiana, minimally invasive procedures are becoming a preferred option.
What Is Uterine Fibroid Embolization
Uterine fibroid embolization, often referred to as UFE, is a minimally invasive procedure performed by interventional radiologists. It works by blocking the blood supply to fibroids, causing them to shrink over time.
How the procedure works
A small catheter is inserted through the groin or wrist
Tiny particles are delivered to fibroid blood vessels
Blood flow to fibroids is reduced
Fibroids gradually shrink and symptoms improve
This approach is widely recognized as a non surgical fibroid treatment in Louisiana, particularly for women who want to avoid major surgery.
Benefits of Uterine Fibroid Embolization
UFE offers several advantages, especially for women focused on preserving uterine health.
Key benefits
Minimally invasive with no large incisions
Shorter recovery time compared to surgery
Preservation of the uterus
Effective reduction in heavy bleeding
Improvement in bulk-related symptoms
For individuals seeking uterine fibroid embolization in Louisiana, understanding these benefits can help in evaluating whether the procedure aligns with personal health goals.
Who May Be a Good Candidate
Not all patients are ideal candidates for every treatment. UFE is generally suitable for women who:
Experience moderate to severe symptoms
Prefer a non-surgical approach
Want to retain their uterus
Have multiple fibroids
A detailed consultation and imaging evaluation are typically required to determine eligibility.
Addressing Heavy Menstrual Bleeding
Heavy menstrual bleeding, also known as menorrhagia, is one of the most common reasons women seek care for fibroids.
Impact of heavy bleeding
Fatigue due to anemia
Disruption of daily activities
Emotional stress
Reduced quality of life
Effective heavy bleeding in periods treatment often involves addressing the underlying fibroids rather than only managing symptoms.
Non-Surgical Fibroid Treatment Options
While uterine fibroid embolization is a leading option, there are additional non-surgical approaches that may be considered depending on the case.
Other options include
Hormonal therapies
Tranexamic acid for bleeding control
Lifestyle and dietary adjustments
However, these methods may provide temporary relief rather than long-term resolution, especially for larger fibroids.
Recovery and What to Expect
Recovery after uterine fibroid embolization is typically quicker than traditional surgery.
Post-procedure expectations
Mild to moderate cramping for a few days
Return to normal activities within one to two weeks
Gradual symptom improvement over several months
Patients are usually monitored through follow-up visits and imaging to assess fibroid shrinkage.
Choosing the Right Fibroid Treatment in Louisiana
Selecting the appropriate treatment requires a balanced understanding of medical needs and personal preferences.
Factors to consider
Severity of symptoms
Desire for future pregnancy
Size and number of fibroids
Recovery time expectations
Access to specialized care
Women exploring fibroid treatment in Louisiana are encouraged to seek comprehensive evaluations to better understand all available options.
Role of Specialized Care
Access to experienced specialists plays an important role in treatment outcomes. Interventional approaches such as uterine fibroid embolization and spinal neuromodulation therapyrequire expertise in image-guided and minimally invasive procedures. Reliable information, accurate diagnosis, and individualized care planning contribute to better decision-making and improved long-term health outcomes.
Conclusion
Fibroid treatment has evolved significantly, offering women more choices than ever before. For those seeking to preserve uterine health, uterine fibroid embolization provides a minimally invasive alternative to traditional surgery.
Understanding the full range of options, including fibroid treatment without surgery in Louisiana, allows women to make informed decisions that align with their health goals and lifestyle. Careful evaluation and guidance from qualified professionals remain essential in choosing the most appropriate path forward. Contact ustoday to schedule a consultation and explore the best treatment options for you.
Frequently Asked Questions
Q1. Is uterine fibroid embolization safe
Uterine fibroid embolization is considered a safe and effective procedure for many women. Like all medical treatments, it carries some risks, but complications are relatively uncommon when performed by trained specialists.
Q2. Can fibroids return after embolization
Fibroids that are treated typically shrink and do not regrow. However, new fibroids may develop over time in some patients.
Q3. How quickly will symptoms improve
Some symptoms, such as heavy bleeding, may improve within the first few cycles. Others, like pelvic pressure, may take a few months as fibroids shrink.
Q4. Is this a good option for treating heavy periods
Yes, uterine fibroid embolization is often used as a heavy bleeding in periods treatment, especially when fibroids are the underlying cause.
Q5. Are there completely non-surgical options available
Yes, several non surgical fibroid treatment options in Louisiana exist, including medications and minimally invasive procedures like embolization.
Q6. Will I need to stay in the hospital
Most embolization procedures are performed as outpatient or short-stay procedures, depending on the patient, depending on individual circumstances.
For many expecting parents, the discovery of fibroids during a routine prenatal ultrasound comes as a surprise.
Fibroids are incredibly common, and in many cases, people don’t even know they have them until pregnancy brings them to light.
As more individuals choose to start families later in life, when fibroids naturally become more frequent, these findings are becoming part of the modern pregnancy experience.
While most pregnancies involving fibroids progress smoothly, their presence can raise understandable questions.
Will they affect the baby’s growth?
Increase the risk of preterm birth?
Lead to pain or complications later in pregnancy?
The answers depend on factors like size, number, and location, and with the right monitoring, many people navigate pregnancy with fibroids without major issues.
In this guide, we’ll explain the impact of fibroids on pregnancy, outline potential risks, describe diagnostic approaches, and provide practical strategies for managing fibroids while pregnant.
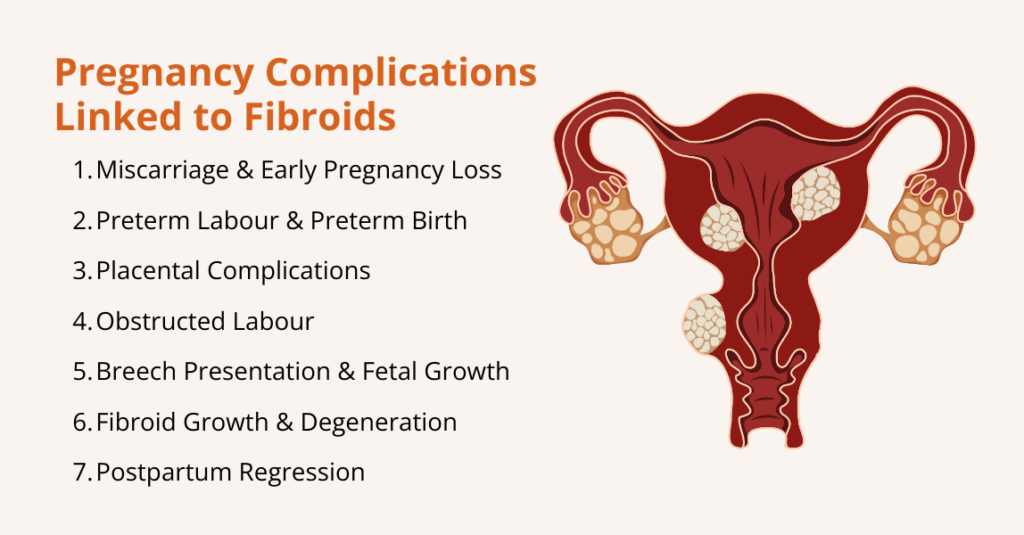
How Fibroids Affect Pregnancy
The presence of uterine fibroids (even when they’ve been harmless before pregnancy) can influence pregnancy in several ways, from early pregnancy loss to complications late in pregnancy or at delivery. The risks vary based on fibroid size, number, and location.
Here are some of the ways fibroids can influence pregnancy:
1. Miscarriage and Early Pregnancy Loss
Fibroids, particularly submucosal lesions, are associated with an increased risk of miscarriage.
A meta‑analysis pooling data from more than 237,000 participants found that women with fibroids had a higher risk of miscarriage than those without fibroids (relative risk RR ≈ 4.5, with miscarriage rates 13.42 % vs. 2.84 % in controls).
The risk is highest when fibroids distort the uterine cavity, because the altered blood supply and mechanical interference impair implantation and early placental development.
2. Preterm Labour and Preterm Birth
Large or multiple fibroids can irritate the uterus and trigger contractions, leading to preterm labour.
A study reported that preterm birth occurred in 12.85 % of pregnant patients with fibroids versus 9.43 % of controls; after adjusting for confounders, fibroids remained associated with preterm birth.
Another study estimated that 10 %–30 % of pregnant women with fibroids develop obstetric complications such as preterm labour. Also, premature uterine contractions may be due to local inflammation, degenerating fibroids, or increased uterine irritability.
3. Placental Issues
Fibroids can interfere with placentation. If a fibroid is located near the placenta, it may lead to:
Placenta Previa: The placenta covers the cervix, obstructing the birth canal.
Placental Abruption: Premature separation of the placenta. The meta‑analysis found an elevated risk of placental abruption in women with fibroids.
Placenta Accreta Spectrum: Fibroids may increase the likelihood of abnormal placental attachment; however, the data remain limited.
4. Need for Caesarean Delivery
Large intramural or subserosal fibroids can physically obstruct the birth canal, preventing the fetal head from descending. Thus, fibroids raise the odds of cesarean delivery.
For example, fibroids growing low in the uterus or near the cervix may block the birth canal, preventing the baby’s head from descending.
Others may distort the uterus, making it harder for the baby to settle into a head-down position and leading to breech or transverse presentations.
5. Breech Presentation and Fetal Growth Restriction
Fibroids, especially those in the lower uterine segment, can distort the uterine cavity and limit space for the fetus. Research highlights that breech presentation or other fetal malposition is more common when fibroids are present, likely because fibroids can alter the shape of the uterine cavity.
Similarly, in analyses comparing by fibroid size, larger fibroids conferred especially high risk of breech presentation and placenta previa.
However, the overall effect on fetal growth remains uncertain because many pregnancies with fibroids result in normal birth weights.
6. Fibroid Growth and Degeneration during Pregnancy
Fibroids behave unpredictably during pregnancy.
A study describes a woman in early pregnancy who arrived with severe abdominal pain, which imaging later confirmed was caused by a degenerating fibroid. This degeneration occurs when a fibroid outgrows its blood supply, leading to tissue ischemia and necrosis.
7. Postpartum Regression
After delivery, many fibroids shrink as hormonal levels decline and the uterus involutes.
A case series found that fibroids decreased in size in 7% of women postpartum and that their volume could shrink by 5% within 6 months.
Ongoing breastfeeding may further promote fibroid regression. Another observational study reported that 37 % of fibroids disappeared postpartum and that breastfeeding was associated with fibroid regression.
What are the Risks and Complications of Fibroids during Pregnancy
While many women with fibroids have healthy pregnancies, these benign growths can sometimes create challenges as the uterus expands and hormonal changes intensify.
Here are the key complications associated with fibroids during pregnancy:
1. Premature Rupture of Membranes
Fibroids can cause uterine irritability, increasing the frequency of contractions and elevating the risk of preterm labour.
The high‑risk pregnancy resource notes that adverse outcomes such as preterm labour and premature rupture of membranes (PROM) are more common when fibroids exceed 10 cm.
The meta‑analysis reported that fibroids were associated with both preterm birth and preterm PROM. Continuous antenatal care with ultrasound monitoring can help detect early cervical changes and manage preterm labour, sometimes using medications such as tocolytics to delay delivery.
2. Heavy Bleeding Due to Placental Problem
Placental problems can cause heavy bleeding and require early delivery or caesarean section. Women with placenta previa are more likely to deliver via caesarean section.
Research shows that placenta previa may manifest as painless vaginal bleeding, often requiring bed rest or early delivery; placental abruption presents with painful bleeding and is an obstetric emergency.
Importantly, fibroids located near the placenta or in the lower uterine segment increase these risks.
3. Obstructed Labour
Large fibroids can obstruct the cervix or lower uterine segment. When the fibroid blocks the birth canal, a caesarean delivery becomes necessary.
Additionally, fibroids may cause dystocia (slow cervical dilation), prolonging labour and increasing the likelihood of operative delivery.
The High‑Risk Pregnancy Information site states that a caesarean section is six times more likely in women with fibroids, highlighting the need for careful intrapartum planning.
4. Postpartum Haemorrhage (PPH)
PPH is excessive bleeding after delivery, often due to uterine atony (failure of the uterus to contract). Fibroids can impede uterine contraction, particularly if they distort the uterine muscle or occupy the uterine wall.
The meta‑analysis found that postpartum haemorrhage occurred in 10.10 % of women with fibroids compared with 3.96 % in controls. Obstetric teams anticipate this risk and prepare for active management of the third stage of labour in women with known fibroids.
5. Preeclampsia and Other Hypertensive Disorders
Emerging evidence indicates a modestly increased risk of preeclampsia (new‑onset hypertension with end‑organ damage) in women with fibroids. The meta‑analysis reported an association between fibroids and preeclampsia.
Although the absolute increase is small, pregnant women with fibroids should be monitored for blood pressure changes.
6. Fetal Malpresentation and Growth Issues
Fibroids can affect how a baby positions itself in the uterus, sometimes leading to malpresentation, when the baby is not head-down at the time of delivery.
For example, large fibroids or those located near the lower uterine segment can physically block the baby from turning into the optimal head-first position, increasing the likelihood of breech or transverse presentation.
In addition, fibroids may influence fetal growth. Large or multiple fibroids can reduce the space available for the baby to grow or interfere with blood flow to the placenta, which can occasionally lead to fetal growth restriction (FGR).
While not all fibroids cause these issues, monitoring fetal position and growth via ultrasounds is crucial to ensure timely interventions if complications arise.
How to Diagnose Fibroids during Pregnancy?
Diagnosing fibroids during pregnancy can be challenging because the growing uterus often makes physical examination unreliable.
As a result, healthcare providers rely primarily on imaging to identify fibroids, determine their size, location, and number, and monitor any changes throughout pregnancy.
Here are the main diagnostic approaches:
Ultrasound (US): Ultrasound is the primary tool for detecting fibroids during pregnancy. Using a transabdominal or transvaginal probe, providers can visualize the uterus, count fibroids, measure their size, and monitor growth. Ultrasound is safe because it uses sound waves rather than radiation.
Magnetic Resonance Imaging (MRI): MRI provides detailed images of uterine tissue when ultrasound is unclear, for example, with large fibroids or fibroids behind the placenta.
Other Tests: Techniques like X-ray, CT scans, hysterosalpingography, and sonohysterograms exist but are rarely used during pregnancy due to radiation exposure.
Surgical Diagnosis: In rare cases when imaging cannot clearly differentiate fibroids from other uterine masses, laparoscopy or hysteroscopy may be performed to visualize the uterus directly. These procedures are generally avoided during pregnancy unless absolutely necessary.
Monitoring Fibroids during Pregnancy
Once diagnosed, fibroids are monitored regularly. Obstetricians often perform ultrasounds at 20 weeks, 32 weeks, and sometimes earlier if symptoms (pain, bleeding, rapid uterine growth) arise.
They assess fibroid size, location relative to the cervix and placenta, and signs of degeneration. Given this, frequent imaging helps detect complications such as placental abruption or fetal growth restriction in a timely manner.
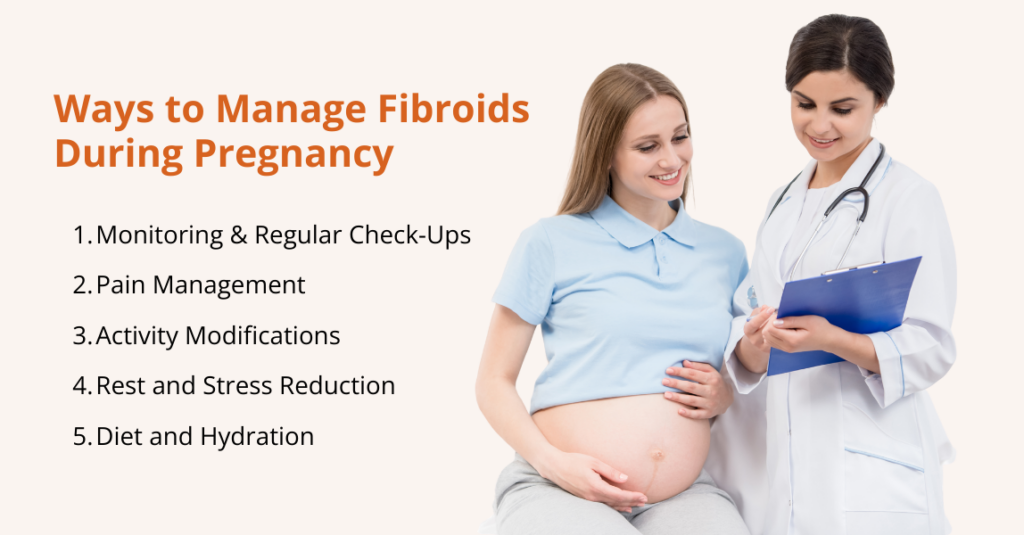
How to Deal with Fibroids during Pregnancy?
Managing fibroids during pregnancy focuses on monitoring for complications, controlling pain, modifying activities, and maintaining overall health.
Here are some of the most common ways to deal with fibroids during pregnancy:
Monitoring and Regular Check-Ups
Once fibroids are diagnosed during pregnancy, ongoing monitoring is essential to ensure both maternal and fetal health.
Regular check-ups help track fibroid growth, assess fetal development, and identify potential complications early. Here’s how:
Routine Ultrasounds: These are performed periodically to track fibroid size, monitor fetal growth, and detect issues such as placental problems or cervical shortening.
MRI when indicated: If ultrasound images are unclear, particularly with large, multiple, or posteriorly located fibroids, MRI can provide more detailed information without radiation exposure.
Fetal Growth Assessments: Serial ultrasounds measure fetal size to identify intrauterine growth restriction (IUGR). If growth concerns arise, obstetricians may adjust delivery planning to ensure optimal outcomes.
Cervical Length Monitoring: Transvaginal ultrasounds measure cervical length, and if the cervix is short, treatments such as progesterone supplementation or cervical cerclage may be recommended.
Regular monitoring ensures that both the mother and baby are closely observed throughout pregnancy, allowing healthcare providers to respond quickly to any complications related to fibroids.
Pain Management
Managing pain safely is crucial to protect both the mother and the developing baby. Treatment strategies should balance effective relief with fetal safety.
If pain or discomfort occurs, acetaminophen (paracetamol) is one of the safest options. According to the American College of Obstetricians and Gynecologists (ACOG), when used as needed, at the lowest effective dose, and for the shortest possible time, acetaminophen remains the preferred pain and fever medicine in pregnancy.
Untreated pain or fever itself can pose risks to a developing baby, so controlling pain wisely matters.
Also, the U.S. Food and Drug Administration (FDA) warns that using NSAIDs after about 20 weeks can harm the baby’s kidneys, reduce the fluid around the baby (amniotic fluid), and lead to serious complications.
Because of these risks, NSAIDs like ibuprofen or naproxen should generally be avoided after mid‑pregnancy, unless a doctor says otherwise.
For mild pain, non‑medication options can also help. Simple measures, such as warm compresses, warm baths or showers, a pregnancy support belt, gentle stretching or prenatal yoga, and rest, can safely ease discomfort.
Activity Modifications
Making thoughtful adjustments to daily activities can help reduce discomfort from fibroids and support a healthy pregnancy.
Gentle modifications, along with proper rest and nutrition, play a key role in managing symptoms safely. Here are the practical tips for activity and lifestyle:
Low-impact exercise: Avoid heavy lifting or high-impact workouts; choose walking, prenatal yoga, or swimming.
Rest and stress management: Use mindfulness, meditation, or prenatal massage to reduce discomfort.
Hydration and diet: Eat a high-fiber, nutrient-rich diet and stay hydrated to prevent constipation and pelvic pressure.
These simple changes help ease symptoms and promote maternal and fetal well-being.
Rest and Stress Reduction
Managing stress and getting adequate rest are important for easing fibroid-related discomfort during pregnancy.
Relaxation Techniques: Practices such as prenatal yoga, deep breathing exercises, and mindfulness can help reduce stress and relieve pelvic or abdominal discomfort caused by fibroids.
Adequate Rest: Prioritizing sufficient rest allows the body to recover, lowers physical strain, and helps minimize pain, especially when fibroids contribute to pelvic pressure.
Incorporating these habits can improve overall comfort and support a healthier pregnancy experience.
Diet and Hydration
Good nutrition and plenty of fluids can ease fibroid-related discomfort and support a healthy pregnancy.
Balanced diet: Eat regular, nutrient-rich meals with plenty of fiber, fruits, vegetables, legumes, and whole grains, plus lean protein and healthy fats. Fiber helps prevent constipation, which can worsen pelvic pressure from fibroids.
Staying hydrated: Drink water throughout the day to support digestion and circulation; staying well hydrated also helps reduce constipation and general discomfort.
Together, a fiber-rich diet and consistent hydration help manage everyday stress and support overall maternal and fetal health.
Frequently Asked Questions (FAQs)
Do fibroids affect pregnancy?
No. Most women with fibroids have normal pregnancies, particularly when fibroids are small or located away from the uterine cavity. The High‑Risk Pregnancy Information site estimates that only 10 %–30 % of pregnant women with fibroids develop complications. Nevertheless, because complications can be serious, women with fibroids should have enhanced prenatal care.
Can fibroids cause pain during pregnancy?
Yes, fibroids can cause pain during pregnancy, and it is the most common symptom associated with these growths. Pain often appears in the second or third trimester when fibroids grow faster than their blood supply, leading to a condition called red degeneration (also known as carneous degeneration). Fibroid pain may also result from mechanical pressure on nearby organs or from torsion of a pedunculated fibroid. Most mild pain can be safely managed with acetaminophen and rest. However, severe or persistent abdominal pain should prompt immediate medical evaluation, as it may indicate complications such as fibroid degeneration, placental issues, or preterm labour.
Do fibroids grow during pregnancy?
Yes, fibroid growth can occur during pregnancy, but patterns vary depending on the size and location of the fibroid. Many fibroids tend to grow in the first trimester due to rising estrogen and progesterone levels. Research shows that small fibroids (less than 1 cm) often increase in volume, medium-sized fibroids usually remain stable, and large fibroids (3 cm or more) may actually shrink. Interestingly, about 10–12% of fibroids regress spontaneously during pregnancy.
Do fibroids shrink after pregnancy?
Yes, many fibroids shrink postpartum. A case series found that fibroid size decreased in 72 % of women after giving birth and that fibroid volume could decrease by 50 % within six months. The postpartum uterus contracts to its pre‑pregnancy size, and hormonal changes (lower estrogen and progesterone levels) contribute to fibroid regression. Breastfeeding may enhance regression. However, some fibroids persist or regrow over time, so postnatal follow‑up is important.
Conclusion
Fibroids are common benign tumors that often coexist with pregnancy. For the majority of women, fibroids will not significantly impact fertility or pregnancy outcome.
Nevertheless, fibroids can increase the risk of miscarriage, preterm labour, placental complications, caesarean delivery, breech presentation, and postpartum haemorrhage.
Comprehensive prenatal care, including regular ultrasounds, growth monitoring, and blood pressure screening, allows obstetricians to detect complications early and implement appropriate interventions.
The safest pain management strategy during pregnancy is to use acetaminophen judiciously after consulting a healthcare professional; NSAIDs should generally be avoided after 20 weeks because they can reduce amniotic fluid and harm the fetus.
Non‑pharmacologic measures such as rest, gentle exercise, hydration, and stress reduction can help alleviate discomfort. Most fibroids regress after birth, especially with breastfeeding.
Given this, women with fibroids should work closely with their healthcare team to develop a personalized care plan.
Frequent nighttime bathroom trips. Difficulty starting urination. A constant feeling that your bladder isn’t empty. If enlarged prostate symptoms are disrupting your daily life, you’re not alone—and you have more treatment options than ever before.
Prostate artery embolization (PAE) represents a revolutionary approach to treating benign prostatic hyperplasia (BPH) that’s changing how men think about prostate treatment. At Seamless Medical Centers, we’re proud to offer this advanced, minimally invasive procedure that provides effective relief without the risks and recovery time of traditional surgery.
Understanding Prostate Artery Embolization
Prostatic artery embolization (PAE) is a minimally invasive treatment that helps improve lower urinary tract symptoms caused by benign prostatic hyperplasia (BPH). The procedure works by reducing blood flow to the enlarged prostate, causing it to shrink and relieving pressure on the urethra.
The PAE process:
Tiny particles are delivered through a small catheter to block specific prostate arteries
Reduced blood flow causes the prostate to gradually shrink
Pressure on the urethra decreases, improving urinary flow
Symptoms improve progressively over weeks to months
Prostatic artery embolization represents an emerging minimally invasive procedure for BPH, offering men an alternative to traditional surgical treatments.
How PAE Compares to Traditional Treatments
The landscape of BPH treatment has evolved dramatically, with PAE offering significant advantages over conventional approaches:
PAE vs. TURP (Transurethral Resection of Prostate)
Doesn’t address the underlying prostate enlargement
PAE advantages:
Addresses the root cause by reducing prostate size
Long-lasting results without daily medication
Minimal ongoing maintenance required
Improves both symptoms and quality of life measures
The Science Behind PAE Effectiveness
Recent research demonstrates PAE’s impressive clinical outcomes. PAE provides more urinary and sexual symptoms benefits than conservative treatment up to 24 months in patients with enlarged prostates who haven’t responded adequately to medication alone.
The PAE Procedure: What to Expect
Understanding the process helps ease anxiety about any medical procedure:
Pre-Procedure Preparation:
Comprehensive evaluation including symptom assessment
Imaging studies to map prostate blood supply
Review of medications and medical history
Discussion of expectations and post-procedure care
During the Procedure:
PAE is performed through a small catheter inserted by your interventional radiologist into the artery in your wrist or groin
Conscious sedation keeps you comfortable throughout
One of PAE’s most appealing aspects is the relatively swift recovery:
First Week:
Some pelvic discomfort or burning during urination
Gradual return to light activities
Temporary urinary frequency possible
Weeks 2-4:
Significant improvement in comfort levels
Return to normal work and daily activities
Initial symptom improvements often noticeable
Months 1-3:
Progressive symptom relief as prostate shrinks
Improved urinary flow and reduced frequency
Enhanced quality of life measures
Long-term (3+ months):
Maximum benefit typically achieved
Sustained symptom relief
Maintained improvement over years
Safety Profile and Side Effects
The PAE procedure has a lower risk of urinary incontinence and sexual side effects (retrograde ejaculation or erectile dysfunction), when compared with more invasive surgical procedures.
Common temporary effects:
Patients may experience “post-PAE syndrome” for days following the procedure, which can include nausea, vomiting, fever, pelvic pain, or painful or frequent urination
These symptoms typically resolve within a week
Serious complications are rare:
Infection requiring antibiotics
Bladder spasm or temporary retention
Bleeding or hematoma at access site
The safety advantage is clear: Studies consistently show lower complication rates compared to surgical alternatives, making PAE an attractive option for men concerned about treatment risks.
Long-Term Outcomes and Satisfaction
Research demonstrates excellent long-term outcomes with PAE:
Symptom improvement:
Sustained reduction in urinary frequency and urgency
Improved urinary flow rates
Better sleep quality due to reduced nighttime urination
Enhanced overall quality of life
Patient satisfaction:
High rates of patient satisfaction and treatment acceptance
Low rates of additional intervention
Most men would recommend PAE to others with similar symptoms
Seamless Medical Centers Advantage
Our board-certified interventional radiologists bring specialized expertise in advanced embolization procedures specifically designed for men’s health needs.
What distinguishes our approach:
Specialized expertise in minimally invasive men’s health procedures
Advanced imaging technology for optimal precision and safety
Comprehensive evaluation to ensure you’re an ideal candidate
Insurance coordination handled by our experienced team
We understand that prostate treatment involves both medical and quality-of-life considerations. PAE should only be performed by knowledgeable and trained interventional radiologists, ensuring you receive the highest standard of care.
Insurance Coverage and Accessibility
PAE is typically less expensive than even other minimally invasive procedures and is covered by most insurance plans, making this advanced treatment accessible to men who need it. PAE offers an effective, minimally invasive solution that addresses the underlying problem while preserving your comfort and lifestyle.
Ready to explore PAE? Contact Seamless Medical Centers to schedule your consultation. Our experienced team will evaluate your specific situation and help determine if PAE is the right choice for your BPH treatment needs.
Individual results may vary. This information is for educational purposes only and should not replace professional medical advice. Treatment decisions should be made in consultation with qualified healthcare providers.
**Excerpt (in the right sidebar):**
Frequent nighttime bathroom trips and difficulty starting urination disrupting your life? PAE offers effective BPH relief without surgery, faster recovery, and fewer side effects.
Experience Relief from Failed Back Surgery Pain at Seamless Medical Centers
You went through back surgery hoping it would finally bring relief. You followed the instructions. You committed to recovery. And yet, the pain is still there.
For many people, persistent pain after spinal surgery is not just physically exhausting — it is emotionally draining. It can feel discouraging, confusing, and even isolating. If you are still struggling with back or leg pain months after surgery, you are not alone. This condition is often referred to as failed back surgery syndrome (FBSS).
At Seamless, we understand how frustrating this experience can be. Our approach is not just about treating symptoms — it is about listening carefully, identifying the true source of pain, and helping you regain control of your life. One advanced treatment option that has helped many patients with FBSS is spinal cord stimulation.
Let’s explore what that means and whether it could be right for you.
What Is Failed Back Surgery Syndrome?
Failed back surgery syndrome does not mean the surgery itself was necessarily done incorrectly. Instead, it describes ongoing or recurring pain after spinal procedures such as discectomy, laminectomy, or spinal fusion.
There are many possible reasons pain may persist, including:
Scar tissue forming around nerves
Incomplete nerve decompression
Recurrent disc herniation
Nerve irritation or damage
Degeneration in nearby spinal segments
An initial diagnosis that did not fully capture the root cause
The pain is often neuropathic, meaning it stems from irritated or damaged nerves. Patients commonly describe it as burning, tingling, stabbing, or shooting pain that radiates into the legs.
Most importantly, it is real. And it deserves thoughtful, compassionate care.
When Traditional Treatments Are Not Enough
Most patients with FBSS try several treatments before exploring advanced options. These may include:
Physical therapy
Anti-inflammatory medications
Opioid medications
Epidural steroid injections
Nerve blocks
Behavioral therapy for coping strategies
While these approaches can be helpful, they do not always provide lasting relief — especially for chronic nerve-related pain.
If you feel like you have “tried everything” and are still struggling, Spinal cord stimulation may offer a different path forward.
What Is Spinal Cord Stimulation?
Spinal cord stimulation is a minimally invasive therapy designed to change how pain signals travel to the brain. A small device, similar to a pacemaker, is placed under the skin. Thin wires called leads deliver gentle electrical impulses to specific areas of the spinal cord.
These impulses modify pain signals before they reach the brain, reducing how strongly pain is perceived. Rather than masking pain with medication, spinal cord stimulation works directly within the nervous system to help calm amplified pain signals.
How It Works in Simple Terms
Think of chronic nerve pain like a faulty alarm system that keeps sounding even when there is no danger.
Spinal cord stimulation helps “turn down the volume” of that alarm.
Depending on the system used, patients may feel:
A mild tingling sensation replacing pain
Or, with newer high-frequency systems, no sensation at all — just reduced pain
The goal is not to numb you, but to help your nervous system communicate more normally again.
What to Expect: A Two-Step Process
One of the most reassuring aspects of spinal cord stimulation is that it begins with a trial phase. During this temporary period, patients can experience the potential pain relief firsthand before committing to a permanent implant, ensuring confidence, comfort, and informed decision-making throughout the treatment process.
Trial Phase
Before committing to a permanent implant, a temporary device is placed to test whether the therapy provides meaningful relief.
During this several-day trial, you will evaluate:
How much your pain improves
Whether daily activities feel easier
Your comfort with the system
This step ensures you have control in the decision-making process.
Permanent Implantation
If the trial is successful, a permanent device is implanted. The procedure typically involves:
Placing leads in the epidural space
Positioning a small pulse generator under the skin
Custom programming to match your pain pattern
It is minimally invasive and usually performed as an outpatient procedure.
Potential Benefits for Patients with FBSS
For the right candidate, spinal cord stimulation can offer meaningful improvements:
Significant Pain Reduction
Many patients experience at least 50 percent pain relief, while some achieve even greater improvement.
Reduced Dependence on Medications
Lower reliance on opioids and other pain medications can reduce long-term side effects and health risks.
Improved Daily Function
Better pain control often allows patients to return to activities they had stopped — walking longer distances, traveling, or simply sleeping more comfortably.
Adjustable and Reversible
Unlike additional spine surgery, spinal cord stimulation is reversible. The device can be adjusted over time or removed if needed.
Is It Safe?
As with any procedure, there are potential risks, including:
Infection
Lead movement
Device malfunction
Discomfort at the implant site
However, careful patient selection and experienced technique significantly reduce these risks. At Seamless, your safety and comfort remain the highest priorities throughout every step.
Who Is a Good Candidate?
Spinal cord stimulation may be appropriate if you:
Have experienced chronic pain for several months or longer
Have not found relief with conservative treatments
Suffer primarily from nerve-related pain
Are not a strong candidate for additional corrective surgery
Are open to completing a trial period
A thorough evaluation — including imaging, medical history review, and sometimes psychological assessment — ensures the treatment aligns with your specific needs.
What the Research Shows
Clinical studies consistently show that spinal cord stimulation can provide:
Meaningful pain reduction
Improved quality of life
Higher satisfaction rates compared to repeat spine surgery in selected patients
While outcomes vary from person to person, it remains one of the most studied and established treatments for persistent neuropathic pain after back surgery.
Living with a Spinal Cord Stimulator
Most patients adjust well to life with a stimulator. You will learn how to:
Use a handheld controller
Adjust settings as needed
Attend follow-up appointments for fine-tuning
It is important to understand that spinal cord stimulation does not cure the underlying structural issue. Instead, it gives you a powerful tool to manage pain more effectively — and often reclaim parts of your life that pain had taken away.
When to Consider This Option
You might consider spinal cord stimulation if:
Your surgery did not deliver the relief you hoped for
Pain continues to interfere with work, sleep, or relationships
You feel discouraged after multiple treatments
You want to explore alternatives before undergoing another surgery
Living with failed back surgery syndrome can feel overwhelming especially after you placed so much hope in your initial procedure. But persistent pain does not mean you are out of options. Spinal cord stimulation offers a different approach, one that focuses on calming the nervous system and restoring comfort rather than repeatedly operating on the spine.
At Seamless, we believe exceptional care begins with listening. If you are struggling with ongoing back or leg pain after surgery, we are here to help you explore your options with clarity, honesty, and genuine compassion. Contact Seamless to schedule a consultation and take the next step toward relief.
Find Relief from Uterine Fibroids at Seamless Medical Centers
Living with uterine fibroids can feel exhausting, frustrating, and at times overwhelming. Heavy periods that disrupt your workday. Cramping that makes you cancel plans. Fatigue caused by blood loss that leaves you feeling drained and not like yourself.
If you’re searching for uterine fibroid treatment in Port Arthur TX, you’re likely not just looking for information, you’re looking for relief, reassurance, and a solution that truly fits your life.
At Seamless, we understand that fibroid symptoms affect more than your body. They impact your confidence, your energy, your relationships, and your peace of mind. That’s why we offer minimally invasive uterine fibroid embolization, a non surgical fibroid treatment designed to relieve symptoms while preserving your uterus and minimizing downtime.
This guide explains your treatment options with clarity and understanding, while recognizing what you’re experiencing.
Understanding Uterine Fibroids
Uterine fibroids (also called leiomyomas) are noncancerous growths that develop within the muscular wall of the uterus.They are incredibly common, especially during reproductive years, yet many women feel alone in their experience.
Some fibroids remain small and symptom-free. Others can significantly interfere with daily life.
Common Fibroid Symptoms
If you are experiencing any of the following, you are not imagining it — and you are not overreacting:
Heavy bleeding during periods
Prolonged menses lasting more than seven days
Pelvic pressure or fullness
Lower back discomfort
Frequent urination
Constipation
Pain during intercourse
Ongoing fatigue
For many women, treatment for heavy bleeding during periods becomes urgent when anemia develops or when everyday life starts revolving around managing menstrual flow.
You deserve more than just coping strategies. You deserve answers.
Why Women Seek Uterine Fibroid Treatment in Port Arthur TX
Many women try medications first. While medications may help temporarily, they often do not address the underlying fibroids themselves.
Traditional surgery — such as hysterectomy or myomectomy — has long been considered the standard solution. However, surgery involves incisions, anesthesia, longer recovery time, and in some cases, removal of the uterus.
For women who want to:
Preserve their uterus
Avoid major surgery
Minimize time away from family or work
Feel heard and supported in their care decisions
Minimally invasive fibroid treatment offers an empowering alternative.
What Is Uterine Fibroid Embolization?
Uterine fibroid embolization (UFE) is a minimally invasive fibroid treatment that works by blocking blood flow to fibroids, causing them to shrink over time.
Instead of surgically removing fibroids or the uterus, this non-surgical fibroid treatment treats fibroids from the inside — through a small catheter placed in an artery.
How the Procedure Works
A tiny incision is made in the wrist or groin.
A thin catheter is guided to the uterine arteries.
Small particles are released to block blood flow to the fibroids.
Over time, the fibroids shrink, and symptoms improve.
The procedure typically takes one to two hours and is performed on an outpatient basis. Most women return home the same day.
There are no large incisions. No hospital stay. No removal of the uterus.
Just targeted treatment focused on restoring your comfort.
Benefits of Minimally Invasive Fibroid Treatment
Choosing uterine fibroid treatment is deeply personal. Many women feel relief simply knowing they have an option that respects both their health and their preferences.
Uterine Preservation
Your uterus remains intact. For many women, this matters emotionally, culturally, or for future fertility considerations.
Outpatient Convenience
You recover at home — in your own space — rather than spending nights in the hospital.
Faster Recovery
Most women resume light activity within a few days and return to normal routines within one to two weeks.
Meaningful Symptom Relief
Women often experience significant improvement in:
Heavy menstrual bleeding
Prolonged menses
Pelvic pressure and discomfort
Energy levels
When bleeding becomes manageable again, many patients describe feeling like themselves for the first time in years.
Who May Be a Candidate for Fibroid Treatment Without Surgery?
You may be a candidate for uterine fibroid embolization if you:
Experience heavy menstrual bleeding
Have prolonged menses
Feel pelvic pressure or discomfort
Prefer to avoid major surgery
Wish to preserve your uterus
A comprehensive evaluation, including imaging such as ultrasound or MRI, ensures that the treatment plan is tailored specifically to you.
At Seamless, your concerns are heard first. The technology comes second.
Finding Relief from Heavy Bleeding and Prolonged Menses
Heavy periods are not something you simply have to endure.
Fibroids can increase the surface area of the uterine lining and interfere with normal contractions, leading to excessive or prolonged bleeding.
Treatment for Heavy Bleeding During Periods
By reducing blood supply to fibroids, uterine fibroid embolization often leads to lighter periods within a few months.
Prolonged Menses Treatment
As fibroids shrink, menstrual cycles typically become shorter and more predictable.
Instead of managing symptoms month after month, this non surgical fibroid treatment addresses the root cause.
What to Expect: Before, During, and After
We know medical procedures can cause anxiety. Understanding the process can bring peace of mind.
Before Treatment
Thorough medical review
Imaging to confirm diagnosis
Honest discussion of risks and benefits
Clear preparation instructions
You will have time to ask questions — and you will receive real answers.
During the Procedure
The procedure is performed under local anesthesia with sedation. You remain comfortable without general anesthesia.
A small bandage covers the insertion site afterward. There are no large scars.
After the Procedure
Some cramping and fatigue are common for a few days. Medication helps manage discomfort.
Over the next several months, fibroids shrink gradually, and symptoms steadily improve.
We stay connected with you through follow-up care to ensure your recovery feels supported every step of the way.
Safety and Long-Term Outcomes
Uterine fibroid embolization is considered safe and effective for appropriately selected patients.
Possible risks may include:
Infection
Temporary menstrual changes
Mild fever or cramping (post embolization syndrome)
Rare complications
Serious complications are uncommon. A detailed consultation ensures you feel confident in your decision.
Many women experience long lasting relief, improved energy, and renewed confidence after treatment.
Choosing Uterine Fibroid Treatment in Port Arthur TX
Choosing treatment is about more than medical outcomes. It’s about how you feel throughout the process.
At Seamless, compassionate care is not an afterthought — it’s the foundation of everything we do. From your first consultation to your final follow-up, our goal is to make you feel:
Heard
Respected
Supported
Fully informed
If fibroid symptoms are interfering with your life, you do not have to continue pushing through the discomfort.
Conclusion
If you’re searching for uterine fibroid treatment in Port Arthur TX, know that relief is possible — and you don’t have to choose between effective treatment and compassionate care.
Minimally invasive uterine fibroid embolization offers a uterine-preserving, outpatient solution for heavy bleeding, prolonged menses, and pelvic discomfort.
At Seamless, we are committed to delivering advanced treatment with exceptional patient care. Contact us today to schedule your consultation and learn whether minimally invasive fibroid treatment is right for you.
Frequently Asked Questions
What is recovery time after uterine fibroid embolization?
Most women return to light activity within a few days and resume normal routines in one to two weeks.
Will my periods stop completely?
The goal is to reduce heavy bleeding and prolonged menses, not eliminate periods entirely.
Is UFE effective for heavy periods?
Yes, uterine fibroid embolization is widely used as treatment for heavy menstrual bleeding when fibroids are the cause.
Can fibroids return?
Treated fibroids typically shrink permanently. However, new fibroids may develop over time.
If your knee hurts, the thought of a full knee replacement can feel big, scary, expensive, and life-changing.
The good news is that a total knee replacement is not the only path.
Many people can ease pain, regain function, and stay active for years with other approaches that delay or even avoid major surgery.
Alternatives range from simple self-care and physical therapy to injections, braces, and newer minimally invasive or joint-preserving procedures.
These options can reduce pain, improve how you move, and, in some cases, protect the joint so you can keep doing the things you love.
However, which option is right depends on the extent of knee damage, your age, activity level, overall health, and your goals.
This article walks through both non-surgical and minimally invasive/joint-preserving options, clearly showing what each can do, its limitations, and the types of patients who typically benefit.
What are Knee Replacement Alternatives?
Knee replacement alternatives are treatments that help reduce knee pain and improve movement without needing a total knee replacement.
These options focus on managing symptoms, supporting the joint, and preserving as much of the natural knee as possible. They’re often used when someone wants to avoid major surgery, isn’t ready for it yet, or only has early-to-moderate joint damage.
Knee replacement alternatives are designed to:
Reduce pain and inflammation: They help reduce swelling in the knee, ease stiffness, and make daily activities more comfortable.
Improve mobility and function: By strengthening surrounding muscles or improving joint lubrication, these treatments help the knee move more smoothly.
Delay or avoid knee replacement surgery: For many people, especially those with moderate arthritis, alternatives can buy valuable time before surgery is needed.
Preserve natural knee structure: Instead of replacing the entire joint, these approaches aim to protect existing cartilage, bone, and ligaments for as long as possible.
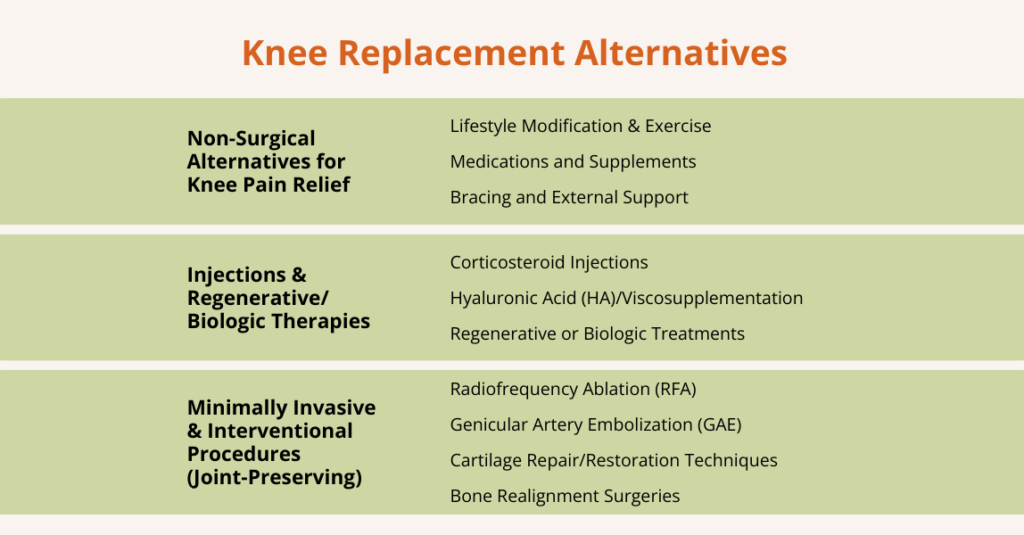
Non-Surgical Alternatives to Knee Replacement
Non-surgical treatments are often the first-line options for managing knee pain, especially in people with early or moderate knee problems. These approaches focus on reducing pain, improving mobility, and preserving joint health without surgery.
Lifestyle Modification & Exercise
One of the most effective ways to manage knee pain without surgery is through lifestyle changes and targeted exercises. These strategies focus on reducing stress on the joint, improving muscle support, and maintaining knee mobility.
Weight Management: Losing excess weight reduces stress on your knee joints. Even a small amount of weight loss can significantly ease pain and slow further joint damage.
Low-Impact Exercise: Activities such as walking, cycling, swimming, water-based exercise, or stationary biking help maintain mobility and keep joints moving without overloading them.
Strengthening & Stability: Guided physical therapy and exercises targeting the quadriceps, hamstrings, and hip stabilizers strengthen muscles around the knee.
Activity Modification: Avoiding high-impact activities such as running or jumping, and replacing them with knee-friendly routines, helps minimize wear and tear while still allowing you to stay active.
Medications and Supplements
For many people, medications and supplements can help manage knee pain alongside lifestyle changes and exercise.
Non‑Steroidal Anti-Inflammatory Drugs (NSAIDs), such as ibuprofen, are commonly used to relieve pain and reduce inflammation. They are effective for short-term symptom management and can help you stay more active.
A systematic review of 146 studies found that most (over 90%) reported positive outcomes for supplements such as glucosamine and Chondroitin sulfate in human joint pain and osteoarthritis, and that these supplements were generally well tolerated.
However, another study found that long-term NSAID use was associated with a significantly greater likelihood of worsened symptoms, including increased pain, stiffness, and disability, compared with non‑users.
That said, NSAIDs are not suitable for everyone and can carry risks, including gastrointestinal irritation or cardiovascular concerns, especially with long-term use. For this reason, medical supervision is important to ensure safe use.
Bracing and External Support
Knee braces are a simple way to support the joint, reduce pain and stiffness, and help you move more confidently. Many people with knee arthritis find them especially helpful for symptom relief and safer activity.
Here’s how it helps:
Reduce pressure on parts of the knee joint
Improve alignment and stability
Decrease pain, stiffness, and improve function
Despite this, braces and external support are not a guarantee. Complications are uncommon but can include skin irritation, pressure sores, or nerve compression.
Injections & Regenerative/Biologic Therapies
Injections and biologic treatments aim to reduce knee pain, improve the joint environment, and help repair or slow the degeneration of tissues.
These therapies are often used when non‑surgical measures (like exercise, weight management, bracing) are not enough, or when someone wants to delay surgery while preserving the joint.
Types of injections & biologic options include:
Corticosteroid Injections
These are anti-inflammatory injections used to calm flare‑ups of arthritis or inflammation inside the knee joint. They can provide short‑ to moderate-term pain relief.
Hyaluronic Acid (HA)/Viscosupplementation
HA injections (joint lubrication shots) provide joint lubrication, reducing friction between joint surfaces. This can ease pain and improve mobility, especially in cases of osteoarthritis.
Regenerative or Biologic Treatments
Platelet-rich plasma (PRP) or stem-cell (mesenchymal stem cell, MSC) injections use the patient’s own biological material to support the knee joint.
These treatments aim to reduce inflammation, support tissue health, and in some cases encourage healing or slow cartilage degeneration.
While outcomes vary, these treatments focus on maintaining knee function and delaying the need for surgery.
These treatments are designed for people who want pain relief and better knee function without going straight to major surgery like a total knee replacement.
Radiofrequency Ablation (RFA)
Radiofrequency Ablation (RFA) is a minimally invasive pain-relief procedure that targets the small sensory nerves around the knee, called genicular nerves.
These nerves carry pain signals from the knee to the brain. In RFA, a specialized needle delivers controlled heat via radiofrequency waves to “deactivate” these nerves, preventing them from sending strong pain signals.
No incisions are usually done under local anesthesia, and most people return to normal activity within a day or two. Many patients experience relief for 6–12 months, sometimes longer.
For this reason, it is useful for delaying or avoiding knee replacement, especially in people who are not ready or not good candidates for surgery.
Genicular Artery Embolization (GAE)
Genicular artery embolization (GAE) is a modern, minimally invasive procedure used to reduce knee pain caused by osteoarthritis. In osteoarthritis, the joint lining becomes inflamed and develops tiny blood vessels that contribute to pain.
During GAE, a doctor (usually an interventional radiologist) guides a small catheter into the blood vessels around the knee and releases tiny particles that block these extra vessels. By reducing abnormal blood flow, inflammation decreases, which can lead to less pain and improved mobility.
Still have significant pain even after trying treatments like medications, physical therapy, weight loss, or injections.
Are not ready, not suitable, or not willing to undergo knee replacement surgery
Therefore, GAE is a promising option for people wanting relief without major surgery.
Cartilage Repair/Restoration Techniques
Cartilage repair procedures are designed to fix or regrow the smooth cartilage that covers the bones inside the knee.
When only a small area of cartilage is damaged, typically from an injury or early wear and tear, these techniques can help restore the surface and protect the joint.
Here’s how these techniques work
One common method is Autologous Chondrocyte Implantation (ACI). In this procedure, a surgeon takes a small sample of healthy cartilage cells from your knee, grows them in a lab, and then implants them back into the damaged area.
Other modern approaches use scaffolds (specialized materials placed inside the defect) or combine scaffolds with biologic therapies to promote new cartilage growth.
These treatments work best in younger, active patients or people who have localized cartilage defects, rather than widespread arthritis. Good knee alignment and healthy surrounding tissue are important for success.
Remember, cartilage repair is not suitable for everyone. Results can vary, recovery takes time, and these procedures are less effective when the entire joint is affected by arthritis.
Bone Realignment Surgeries
Bone realignment surgery, commonly called an osteotomy, is a joint-preserving procedure used when knee pain is caused by uneven weight-bearing. In many people, arthritis or wear-and-tear affects just one side of the knee.
This occurs when the leg is slightly angled inward (knock-knee) or outward (bow-legged), which increases pressure on one compartment of the joint.
An osteotomy reshapes or cuts the bone (usually the tibia or femur) to realign the leg. This shifts your body weight away from the damaged side and distributes it more evenly across the knee.
Different types of osteotomy include:
High Tibial Osteotomy (HTO): Realigns the shin bone; commonly used when the inner (medial) side of the knee is worn down.
Distal Femoral Osteotomy (DFO): Realigns the thigh bone; often used when the outer (lateral) side of the knee is affected.
Opening-Wedge or Closing-Wedge Techniques: The surgeon either opens a small gap (and fills it with bone graft or plate) or removes a wedge of bone to achieve proper alignment.
Osteotomy is generally recommended for younger or middle-aged adults who still want to stay active but have knee pain from arthritis. It works best for people whose arthritis affects only one side of the knee rather than the entire joint.
Although osteotomy can be very effective, recovery typically takes several months because the bone needs time to heal after repositioning. Thus, it is not the best option for people with severe arthritis affecting the entire knee.
What Are the Pros and Cons of Knee Replacement Alternatives?
Understanding the pros and cons of knee replacement alternatives helps patients choose the option that best matches their condition, goals, and lifestyle.
Pros
Cons/Limitations
Less invasive or non-invasive, lower risk than total knee replacement (less surgical trauma, lower infection risk).
Often, temporary relief may require repeat treatments (e.g., injections, RFA).
Shorter recovery time, faster return to routine activities than after major surgery.
Effectiveness varies by arthritis severity, alignment, weight, and overall joint condition.
Joint-preserving, keeps your natural knee anatomy and movement.
Regenerative therapies are still evolving; long-term evidence for cartilage regrowth is limited.
Flexible treatment combinations can combine therapies or use them step by step before surgery.
Not suitable for everyone, severe “bone-on-bone,” major deformity, or advanced arthritis may not respond well.
Can delay or avoid knee replacement; ideal for younger, active adults who want to protect their joint.
Access limitations. Advanced cartilage repair procedures may be available only at select centres.
How to Decide if a Knee Replacement Alternative Is Right for You?
When facing knee problems or arthritis, it helps to follow a step-by-step, thoughtful decision-making process rather than jumping straight to major surgery.
The process often begins with the simplest, lowest-risk approaches and progresses only if symptoms persist or worsen, balancing benefit, risk, and each patient’s goals for their knee and lifestyle.
1. Start with Initial Evaluation & Conservative Management
At first, most patients begin with non-surgical care, such as lifestyle changes, physical therapy, or structured exercise, bracing or knee support, and, if appropriate, medications (such as NSAIDs).
These interventions aim to reduce joint load, strengthen surrounding muscles, improve mobility, and reduce pain, often with minimal risk and without surgery.
2. If Symptoms Persist or the Arthritis is Moderate
Consider additional therapies, such as injections or, if appropriate, regenerative/biologic therapies. These can sometimes provide greater relief or slow disease progression when conservative care alone isn’t sufficient.
3. If Pain/Function Limitations Despite Conservative & Injectables
In this case, more invasive procedures may be evaluated, such as nerve-targeting procedures or other pain-management approaches.
This makes sense, particularly if surgery is risky or if the patient wants to postpone a full knee replacement while still maintaining mobility and quality of life.
4. If Structural Damage Is Localized/Partial
In this situation, cartilage repair/restoration procedures, partial joint procedures, or bone-realignment surgery (osteotomy) may be considered, depending on alignment, cartilage health, and the patient’s activity goals.
5. Monitor & Reassess
Whatever path is chosen, conservative, injectable, interventional, or surgical, regular follow-up is essential. This includes clinical check-ups and imaging when necessary.
As arthritis progresses or the joint condition changes, treatment goals may shift, and at some point, a more definitive procedure (such as joint replacement) may become the best option.
How Do You Choose the Right Alternative to Knee Replacement?
Choosing a non-surgical, minimally invasive, or joint-preserving option depends on the person and the knee.
Here are some key aspects to consider when deciding which options fit best:
1. Stage of Disease
These alternatives work best when arthritis or cartilage loss is mild to moderate, meaning enough of the joint surface remains intact.
If the damage is limited, treatments like injections, bracing, cartilage repair, or osteotomy can relieve symptoms and protect the joint. When arthritis is widespread and severe, however, joint replacement is often the more reliable solution.
2. Age and Activity Level
Younger or more active patients often benefit most from joint-preserving and regenerative options, as preserving natural cartilage and bone helps them remain active longer.
Older patients or those seeking a definitive, long-lasting fix may lean toward replacement, but age alone shouldn’t rule anyone out; overall health and goals matter, too.
3. Patient’s Health and Surgical Risk
For people with other health problems (for example, heart or lung disease), or those who are poor candidates for major surgery, minimally invasive choices are attractive because they carry lower surgical risk and shorter recovery.
These options give symptom relief while avoiding the stress of a major operation.
4. Symptom Severity and Goals
If the main goal is to reduce pain, improve function, and delay a major operation rather than immediately replace the knee, conservative and interventional options are appropriate.
Patients with severe, constant pain that limits daily life despite other treatments may still need replacement sooner.
5. Patient Preferences
Patient values and priorities matter. Some people prefer less invasive treatments first, even if results might be temporary, to avoid major surgery.
Others prefer a single, durable solution and accept the tradeoffs of joint replacement. However, good decision-making balances the likely benefits and risks and considers how each option fits the patient’s lifestyle and goals.
Frequently Asked Questions (FAQs)
Is there an alternative to knee replacement surgery?
Yes, there are several alternatives to knee replacement, depending on the severity of your knee arthritis and your goals. The main types of alternatives include:
There isn’t a single “best” alternative to knee replacement; the right choice depends on your knee’s condition, age, activity level, and personal goals. For early or moderate arthritis, starting with conservative measures like weight management, physical therapy, bracing, and NSAIDs is usually effective. If pain persists, injections such as corticosteroids, hyaluronic acid, or biologic treatments like PRP can provide additional relief. For patients who want pain control without major surgery, minimally invasive options like radiofrequency ablation or genicular artery embolization may help. Younger or active patients with localized cartilage damage or malalignment may benefit from joint-preserving procedures such as cartilage repair or osteotomy.
How can I fix my knees without surgery?
You can manage knee problems without surgery by managing your weight, engaging in low-impact exercise, and undergoing physical therapy to strengthen and support the joint. Knee braces can improve alignment and reduce pain, while medications or injections (NSAIDs, corticosteroids, hyaluronic acid, or PRP) help control inflammation.
For persistent pain, minimally invasive procedures like radiofrequency ablation or genicular artery embolization may be options. In some cases, joint-preserving surgeries such as cartilage repair or osteotomy can preserve function and delay replacement. Regular monitoring and activity adjustments are key to staying active and managing symptoms.
What is the new procedure instead of knee surgery?
The newest non-surgical procedure for knee pain is Genicular Artery Embolization (GAE). In this minimally invasive treatment, a doctor blocks the small blood vessels (genicular arteries) that supply the inflamed tissue. By reducing abnormal blood flow, GAE helps decrease inflammation, relieve pain, and improve function, especially for people with moderate knee arthritis who want to avoid or delay knee replacement. The procedure is performed through a small incision, usually in an outpatient setting, and allows for a faster recovery than traditional surgery while preserving the knee’s natural structure.
Is there a way to avoid a knee replacement?
Yes, in many cases, you can avoid or delay a knee replacement. It depends largely on the severity of joint damage, your age, lifestyle, and how much you’re willing to invest in care and maintenance. Here’s how:
Lifestyle & Exercise: Lose excess weight, do low-impact exercises, and strengthen knee-supporting muscles.
Physical Therapy & Bracing: Stabilize the joint, improve mobility, and reduce pain.
Injections / Lubrication: Corticosteroids or hyaluronic acid to ease pain and improve joint movement.
Regenerative Therapies: PRP or stem-cell injections to reduce inflammation and support tissue healing.
These approaches can help manage symptoms, preserve joint function, and delay surgery, depending on your knee’s condition and overall health.
How to avoid knee surgery naturally?
Many people can manage knee pain and protect their joints without surgery by making smart lifestyle choices and adopting natural strategies that reduce stress on the knee, strengthen supporting muscles, and improve joint health.
Here are some ways to avoid knee surgery naturally:
Keep a Healthy Weight: Less weight reduces pressure on the knees and slows joint wear.
Strengthen Supporting Muscles: Strong quadriceps, hamstrings, and hip muscles help stabilize the knee.
Low‑Impact Exercise: Walking, cycling, swimming, or yoga maintains mobility without overloading the joint.
These approaches won’t reverse severe arthritis, but they can slow progression, ease pain, and help you stay active longer.
Conclusion
If you’re looking to manage knee pain without jumping straight to surgery, there are many options available.
From lifestyle changes and exercises to injections, biologic treatments, and minimally invasive procedures, these approaches can help reduce pain, improve movement, and protect your natural knee.
These alternatives are especially helpful if your arthritis is mild to moderate, if you’re younger or active, or if you just want to delay or avoid major surgery.
Remember, there’s no single best solution; the right choice depends on your knee, your health, and your goals.
The best way to decide is to discuss with your healthcare team. Your doctor, physiotherapist, or interventional specialist can help you determine which options are right for you and in the right order so that you can stay active and comfortable for as long as possible.
Do you find yourself running to the bathroom more often than usual, even disrupting your day or sleep?
Most healthy adults urinate about 6–8 times a day, so going more than eight times, or waking repeatedly at night (nocturia), can feel frustrating and inconvenient.
Sometimes, frequent urination is harmless, like during pregnancy or after drinking a lot of fluids. However, it can also indicate an underlying health issue.
This guide breaks down why frequent urination happens in both women and men, the symptoms to watch for, practical self-care tips, and available medical treatments.
What is Frequent Urination?
Frequent urination means needing to pee more often than usual during the day or at night. It can be annoying and disruptive, and it is a common issue experienced by many people.
For example, waking up more than twice at night to void (nocturia) is generally beyond the normal range. Urinating more than 8 times per day falls into the “frequent urination” range.
In contrast, most healthy adults urinate 6–8 times per day (roughly every 3–4 hours) and wake only once at night at most.
Needing to urinate much more often than this, especially if it suddenly increases, can be a sign of conditions ranging from mild (such as increased fluid intake) to serious (such as infections, metabolic or neurologic disease).
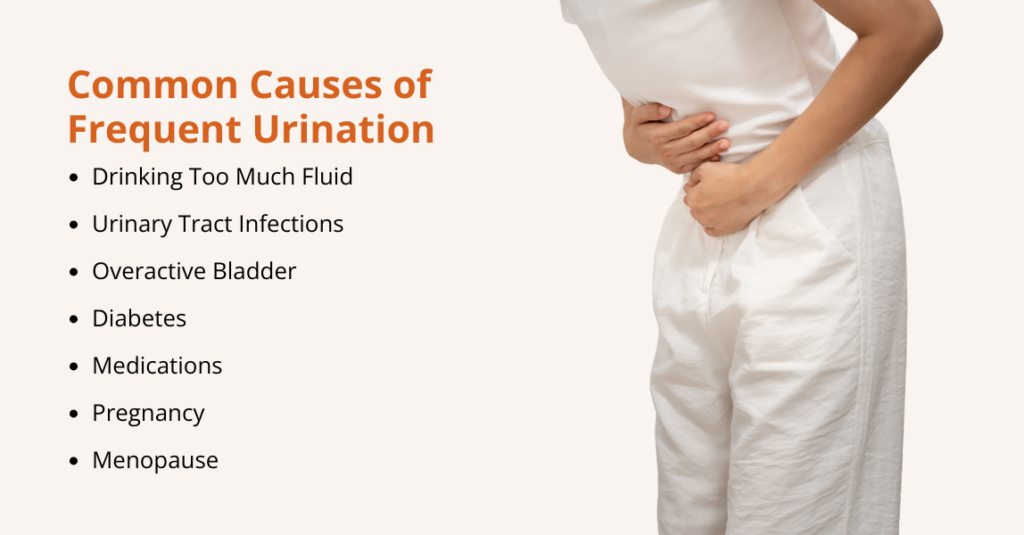
What Causes Frequent Urination?
Frequent urination can result from many different factors. Common causes include:
Drinking too Much Fluid: If you drink a lot, especially coffee, tea, energy drinks, or alcohol, you empty your bladder more quickly.
Urinary Tract Infections (UTIs): A UTI irritates the bladder lining and triggers a strong, repeated urge to pee. People often feel a burning sensation, need to pee even when little comes out, or notice cloudy or bloody urine.
Overactive Bladder (OAB): With OAB, the bladder muscles suddenly contract, causing urgency and frequent trips to the bathroom, even if the bladder isn’t full.
Diabetes: High blood sugar causes extra glucose to spill into the urine, pulling more water with it. This leads to passing large amounts of urine and feeling thirsty all the time.
Medications (Diuretics): “Water pills” used for high blood pressure or swelling make the kidneys release more salt and water, so you pee more.
Pregnancy: The uterus presses on the bladder, and the kidneys work harder, leading to more frequent urination.
Menopause: Lower estrogen levels weaken bladder tissues and increase the risk of UTIs, urgency, and leakage.
Anything that fills or irritates the bladder can increase urination frequency, and understanding these causes is the first step toward appropriate treatment.
Causes of Frequent Urination in Women
Women experience frequent urination for several gender-specific reasons. Key female causes and risk factors include:
Pregnancy: Hormonal changes, increased urine production, and pressure from the growing uterus make frequent urination very common, especially in the first and third trimesters.
Menopause: Lower estrogen weakens bladder and urethral tissues, leading to urgency, leakage, and a higher risk of UTIs, which can trigger sudden, frequent urination.
Urinary Tract Infections (UTIs): Because women have a shorter urethra, bacteria reach the bladder more easily. UTIs cause repeated urges to pee, burning, and small amounts.
Overactive Bladder (OAB): Women are slightly more likely to develop OAB, which causes sudden urges and frequent daytime and nighttime urination.
Pelvic Floor Dysfunction: Pregnancy, childbirth, or surgery can weaken pelvic floor muscles, causing urgency, leaks, and the need to urinate more often.
Causes of Frequent Urination in Men
Men can have frequent urination for some causes unique to males, in addition to the general factors above (like fluid intake or diabetes). Important male-specific causes include:
Benign Prostatic Hyperplasia (BPH): The prostate enlarges with age and presses on the urethra, causing weak flow, incomplete emptying, and frequent or nighttime urination.
Prostatitis: Inflammation of the prostate leads to pelvic pain, burning with urination, and repeated urges to pee, often with a feeling of not emptying fully.
Urinary Tract Infections (UTIs): Less common in men, but when present, they cause urgency, burning, frequent urination, and sometimes blood, often linked to prostate issues.
Bladder Stones: More common in men, especially when bladder emptying is poor. Stones irritate the bladder wall, causing frequent urination, urgency, pain, or hematuria.
Diabetes: Hyperglycemia leads to increased urine production. Men with uncontrolled diabetes may notice increased thirst, large urine volumes, and frequent nighttime urination.
Frequent Urination Treatment Options
When lifestyle and behavioral changes are insufficient, or when there is an underlying medical cause, medical treatment may be necessary.
Here are the most common treatment options:
Medications
These treatments help manage urgency, frequency, and bladder control by addressing the specific cause of symptoms.
Anticholinergics & Beta-3 Agonists: Used for overactive bladder. Anticholinergics block bladder muscle contractions; beta-3 agonists relax the bladder.
Alpha-Blockers: For men with BPH. They relax the prostate and the bladder neck to improve urine flow.
5-Alpha-Reductase Inhibitors: Long-term BPH treatment that shrinks the prostate and reduces urinary symptoms.
Diuretics: Increase urination; timing may be adjusted if they cause bothersome frequency.
Topical Estrogen: Helps postmenopausal women by improving vaginal and urethral tissue health and reducing urgency.
Bladder and Behavioral Therapies
These are non-surgical approaches that focus on training and strengthening the bladder and pelvic muscles to improve control and reduce frequent urination or incontinence:
Bladder Training: This method helps you gradually increase the interval, enabling the bladder to hold more urine and reducing urgency and frequency.
Pelvic Floor Exercises (Kegel Exercises): These exercises strengthen the pelvic floor muscles, which support the bladder and urethra.
Biofeedback: Biofeedback uses sensors or devices to help you see how your pelvic muscles are working. It guides you in contracting and relaxing the right muscles.
These therapies are often used in combination and guided by a healthcare professional to achieve optimal results.
Minimally Invasive Procedures
These treatments offer non-surgical options for managing urinary problems:
Tiny particles are injected to block blood flow, causing the prostate to shrink over time. This relieves pressure on the urethra, improving urine flow and reducing the frequency of urination. The procedure is done without surgery, often as an outpatient treatment, and has a short recovery time.
Bladder Botox (OnabotulinumtoxinA)
This is used for refractory overactive bladder. Under anesthesia, Botox is injected directly into multiple sites in the bladder wall. The toxin paralyzes part of the bladder muscle, reducing involuntary contractions.
Botox can prevent bladder contractions, providing symptom relief for approximately 6–9 months. However, periodic re-injections may be needed.
Surgical Interventions
When medications and minimally invasive treatments aren’t enough, surgical options can help relieve urinary symptoms and improve bladder control.
Prostate Surgery
For severe BPH, procedures like Transurethral Resection of the Prostate (TURP) or laser prostatectomy remove excess prostate tissue, opening the urinary channel. This often significantly reduces urinary frequency by relieving bladder obstruction.
Anti-Incontinence Surgery
For women with stress urinary incontinence (UI), procedures like mid-urethral slings or bladder neck suspensions support the urethra, preventing leaks. By reducing incontinence, these surgeries can also improve overall bladder habits.
Neuromodulation Devices
For refractory cases of overactive bladder, sacral nerve stimulators (InterStim) or tibial nerve stimulators (PTNS) deliver mild electrical pulses to modulate bladder activity. These advanced therapies are used when medications and conservative treatments fail.
Remember, each treatment plan is individualized. A doctor will consider the severity of symptoms, the underlying cause, patient preferences, and health.
For example, a young woman with mild OAB may do well with Kegel exercises and bladder training alone, while an older man with BPH may need medications or even surgery for relief.
How to Stop Frequent Urination?
If frequent urination is due to lifestyle factors or an overactive bladder, several self-care strategies can help strengthen bladder control and reduce frequency.
Many of these are first-line recommendations before or alongside medications:
1. Bladder Training
This involves gradually extending the time between bathroom visits.
For example, if you are going every 30 minutes out of habit or urgency, you might try delaying for 5 minutes, then 10, then longer, gradually increasing bladder capacity.
Over days or weeks, this can condition the bladder to hold more urine and reduce the number of trips. Bladder training is widely recommended as a first-line therapy for an overactive bladder.
2. Scheduled Bathroom Breaks
Similar to bladder training, setting a regular voiding schedule can help. For example, try urinating at predetermined intervals (e.g., every 2–3 hours) even if you don’t feel a strong urge yet.
This prevents “sudden” emergencies and helps your bladder get used to holding urine. It can also help you track how often you truly need to go and whether you are going out of habit.
3. Pelvic Floor Exercises (Kegels)
The pelvic floor muscles support the bladder and help control urination. Strengthening these muscles can reduce urgency and incontinence.
To do Kegel exercises, simply tighten (squeeze) the muscles you would use to stop the flow of urine, hold for a few seconds, then relax. Repeat 10–15 times per session, several times a day. Over the course of weeks, this can markedly improve control.
4. Reducing Fluid Intake (Especially at Night)
Limit evening beverages, so you’re not forcing the kidneys to produce excessive urine before bedtime. This helps reduce nocturia (nighttime trips). Additionally, avoid excessive daily fluid intake if your bladder is overly sensitive.
Importantly, do not overrestrict fluid intake; staying hydrated is necessary, but avoid drinking a liter right before bed. Similarly, cut back on caffeine (coffee, tea, sodas) and alcohol, as both act as diuretics and bladder irritants.
5. Avoiding Bladder Irritants
Certain foods and drinks can irritate the bladder lining and exacerbate urgency.
The most common offenders include spicy foods, citrus fruits/juices, tomatoes, carbonated drinks, and artificial sweeteners. If you notice a surge in frequency after spicy meals or coffee, try eliminating these triggers.
6. Double Voiding
Especially useful if you feel the bladder is not fully emptying. After you finish peeing, wait a minute or two, then try to pee again. Sometimes this second attempt will release a small additional amount that was left behind.
With time, emptying the bladder more completely may reduce the sensation of fullness that leads to multiple trips.
7. Stress and Anxiety Management
Stress can worsen urinary frequency (due to the “fight or flight” response and pelvic muscle tension).
If you find yourself rushing to the bathroom whenever you feel even a little stress, consider stress reduction exercises. Practice relaxation techniques like deep breathing, mindfulness meditation, or yoga to reduce anxiety.
With these self-help methods, many people see improvement. However, it is important to track progress and provide relevant information if you later require a medical evaluation.
Frequently Asked Questions (FAQs)
How does drinking too much fluid lead to frequent urination?
Drinking large volumes of any fluid increases urine production. Think of the kidneys as filtering blood: the more fluid you drink, the more they filter, and the more urine is produced. This is especially true for beverages with diuretic effects, like coffee and alcohol. In effect, these fluids increase the amount of water in your bloodstream that needs to be excreted.
Why do I feel like I have to pee every 5 minutes?
Feeling like you need to pee every few minutes can be caused by an overactive bladder, which triggers sudden “gotta go” urges and frequent bathroom trips, or a urinary tract infection, which often brings burning, urgency, and discomfort. Certain medications, such as diuretics, can also increase urination. If you experience other symptoms such as pain, fever, or burning, it’s important to see a physician for proper evaluation.
Why am I peeing so much all of a sudden?
A sudden change in frequency of urination suggests a new factor. Common causes include urinary infections and diabetes. For example, a bladder infection can develop quickly and irritate your bladder, causing urgency every few minutes. New-onset diabetes can also cause a rapid increase in urination. It’s also worth reviewing any new medications or dietary changes (e.g., starting caffeine or supplements) that could be affecting your bladder. If the frequent urination is sudden and accompanied by other symptoms (e.g., thirst, sugar cravings), checking blood glucose and urine for infection may be prudent.
When should I worry about peeing a lot?
You should worry and see a healthcare provider if frequent urination comes with concerning symptoms or seriously affects your daily life. Red flags include pain or burning while urinating, blood in the urine, fever, or a sudden, sharp increase in how often you go. Waking up multiple times at night, particularly if it disrupts sleep and daytime functioning, warrants evaluation. Any warning signs, such as pain, fever, blood in the urine, or unusual discharge, require prompt medical attention.
Is it normal to urinate every 2 hours?
Urinating every 2 hours can be normal for someone drinking a lot or with bladder training, but it’s more frequent than the average of 6-8 times a day (every 3-4 hours). Normal frequency depends on your fluid intake and the size of your bladder. If there are no other symptoms, it may not need worrying. But if it’s more frequent than usual for you, or you feel urgency or discomfort, it may need further attention.
Is it normal to pee every 30 minutes?
No, peeing every 30 minutes is far outside the normal range for adults. Going every half hour suggests a serious problem, possibly a bladder infection, severely overactive bladder, or other issue. It should be evaluated by a doctor.
When should someone see a doctor for frequent urination?
You should consult a doctor if you urinate more than 8 times a day or wake frequently at night, especially if it disrupts your daily life or comes with other symptoms. These may indicate infections (like UTIs), diabetes, kidney problems, or other serious conditions. Also, see a doctor if you experience any of the following signs:
Pain/Burning: Discomfort while urinating (dysuria).
Blood in Urine: Urine appears pink, red, or brown (hematuria).
Signs of Infection: Fever, chills, cloudy urine, or lower back/side pain.
Urgency & Incontinence: Sudden, uncontrollable need to urinate or leaking urine.
Nocturia: Waking more than once or twice at night, disrupting sleep.
Systemic Symptoms: Excessive thirst or hunger, fatigue, or unexplained weight loss.
Difficulty Urinating: Trouble starting, weak stream, or feeling of incomplete emptying.
Conclusion
Frequent urination is a common condition with a wide range of causes. In some cases, it may simply result from drinking large amounts of fluids or consuming diuretics such as caffeine and alcohol.
However, it can also indicate more serious medical issues, including urinary tract infections (UTIs), diabetes, an overactive bladder, or prostate enlargement in men.
Therefore, understanding the context and symptoms is essential. New, sudden, or severe increases in urination, especially when combined with pain, burning, blood in the urine, fever, or other systemic symptoms, should prompt timely medical evaluation.
For many people, non-invasive options such as behavioral and bladder therapies, like bladder training, Kegel exercises, and fluid management, can significantly improve symptoms. In other cases, medications may help manage an overactive bladder, prostate issues, or infections.
For persistent or severe problems, minimally invasive procedures or surgical interventions may be necessary to relieve obstruction or restore bladder function.
Importantly, early evaluation and intervention can prevent complications. With the right combination of lifestyle adjustments, medical treatment, or procedures, most people experience meaningful improvements in urinary frequency and quality of life.
A swollen knee, often called knee effusion, means extra fluid has collected inside the joint or in the tissues that surround it.
Because the knee is a large hinge joint that supports your body weight and allows a wide range of motion, even mild swelling can be painful and make walking or bending difficult.
Swelling may occur suddenly after a traumatic injury, or it can develop gradually as the result of chronic inflammation or degenerative disease.
Although swelling itself is not a diagnosis, it is an important warning sign that something else is wrong. Causes range from minor sprains and ligament tears to more serious problems such as infections or autoimmune conditions.
In the United States, knee injuries account for over half a million emergency department visits each year, and the lifetime prevalence of knee swelling is estimated at 27%. These numbers show how common knee problems are and why prompt attention matters.
This guide walks through what a swollen knee is, its common causes and risk factors, symptoms to watch for, possible complications, how clinicians diagnose it, evidence-based treatment options, and practical steps you can take to reduce the risk of recurrence.
What is a Swollen Knee?
Knee swelling happens when extra fluid builds up in or around the knee joint. The knee connects your thigh bone (femur) to your shin bone (tibia) and kneecap (patella).
It’s the largest joint in your body, supported by cartilage, muscles, ligaments, and nerves. Because so many structures work together, anything that irritates or injures the knee can lead to swelling.
Swelling can occur after an injury or develop due to an underlying health condition affecting the tissues around the joint.
When your knee is swollen, you may also notice:
Knee pain
Stiffness or a tight feeling
Redness or discoloration
Warmth or heat around the joint
Most mild cases can be managed at home with rest, ice, elevation, and over-the-counter (OTC) medicine.
However, you should see a healthcare provider if the swelling follows a fall or sports injury, doesn’t improve after a few days, causes severe pain, or makes it hard to move your knee.
What Causes a Swollen Knee?
Since swelling is a symptom, not a condition in itself, it can result from a wide range of underlying conditions.
Here are the key causes of a swollen knee:
1. Traumatic Injuries
Trauma is a leading cause of acute knee swelling. Injuries often occur during sports, falls, or motor vehicle collisions. When soft tissues or bone structures in the knee are damaged, blood vessels rupture, and synovial membrane irritation leads to effusion.
These include:
Ligament Injuries
Ligament tears, especially of the anterior cruciate ligament (ACL), are a leading cause of acute swelling. ACL injuries often happen with a sudden pivot or landing, and people commonly report an audible “pop,” sharp pain, rapid swelling within hours, and a feeling that the knee will give way.
A systematic review indicates that ACL tears often accompany bone bruises, meniscus damage, or cartilage injury, all of which can lead to bleeding or joint fluid build-up (hemarthrosis), a common cause of swelling.
Whereas posterior cruciate ligament (PCL) injuries are less common but produce similar symptoms: pain, rapid swelling, stiffness, and difficulty walking.
Meniscal Tears
The menisci are crescent-shaped cartilage cushions between the femur and tibia.
A twisting injury can tear a meniscus, causing pain, stiffness, swelling, difficulty fully straightening the knee, and occasional locking or catching.
Fractures
Breaks involving the patella, distal femur, or proximal tibia can lead to substantial swelling because bone bleeding often fills the joint space (hemarthrosis).
If the patient cannot bear weight or the leg looks deformed, prompt X-rays or CT scans are essential.
Dislocations
Patellar dislocation, when the kneecap slips out of its groove, is relatively common and causes sudden pain, visible deformity, and swelling.
2. Inflammatory Conditions
Inflammatory arthritides can provoke episodic or chronic knee swelling. They result from autoimmune processes or crystal deposition within the synovium.
Rheumatoid Arthritis (RA)
Rheumatoid arthritis is a systemic autoimmune disease that causes chronic inflammation of the synovial lining. Although it usually starts in the small joints of the hands and feet, larger joints, including the knee, are frequently affected.
Gout is caused by the deposition of monosodium urate crystals in joints due to hyperuricemia. While the big toe is the classic site, gout can also affect the knees, ankles, and wrists.
Whereas Pseudogout, also called calcium pyrophosphate deposition disease (CPPD), involves deposition of calcium pyrophosphate crystals in articular cartilage and soft tissues. Flares mimic gout but are more likely to involve the knees and wrists.
Septic Arthritis
Septic arthritis is an infection of the joint space, most commonly caused by bacteria. Pathogens enter the knee through hematogenous spread, direct inoculation (trauma or surgery), or extension from osteomyelitis.
Research shows that if a knee injury with hemarthrosis is not treated promptly or properly, patients face a significantly higher risk of developing knee osteoarthritis over the next 10 to 12 years.
The knee becomes extremely painful, swollen, warm, and difficult to move, and patients often have fever or systemic signs of infection.
Viral Arthritis
Acute viral infections can cause transient arthritis due to immune activation and direct viral invasion. Common culprits include parvovirus B19, hepatitis B and C, Epstein–Barr virus, chikungunya, rubella, and arthropod‑borne viruses.
Viral arthritis is acute, generalized inflammation of joints triggered by a broad range of viruses; it presents with joint pain, swelling, fever, rash, and fatigue, and usually resolves spontaneously once the infection is cleared.
3. Degenerative Conditions
Degenerative processes gradually erode joint structures, leading to chronic swelling.
Osteoarthritis
Osteoarthritis is the most common cause of chronic knee swelling. It develops as cartilage breaks down and the joint becomes inflamed.
OA affects over 32 million U.S. adults and is most common in people aged 55–64, though many younger adults are also affected.
Typical symptoms include gradual pain that worsens with activity, stiffness after rest, creaking sensations, and occasional fluid buildup.
Patellofemoral Pain Syndrome (PFPS)
Often called “runner’s knee,” PFPS causes pain at the front of the knee due to irritation in the patellofemoral joint.
People may notice a dull ache, discomfort with running or climbing stairs, pain after sitting, and sometimes mild swelling after activity. Also, overuse, muscle imbalance, poor alignment, and improper footwear are common triggers.
Bursitis
The knee contains several small bursae that reduce friction. Repetitive kneeling, irritation, or infection can inflame these sacs, leading to prepatellar or infrapatellar bursitis. Symptoms include localized swelling, tenderness, and warmth.
4. Infectious Conditions
In addition to septic arthritis and bursitis, infections caused by atypical organisms, such as fungi or mycobacteria, can cause joint swelling, especially in people with weakened immune systems.
These infections may develop more slowly or present with less typical symptoms, so prompt joint aspiration, culture, and targeted (culture-directed) treatment are essential to prevent ongoing damage.
5. Other Systemic Causes
Some systemic diseases can lead to knee swelling through immune or metabolic processes.
Systemic Lupus Erythematosus (SLE)
SLE is an autoimmune condition that can affect multiple organs, including the joints. Around 95% of patients experience joint pain or arthritis, often involving large joints like the knees.
Lyme Disease
Lyme arthritis is caused by infection with Borrelia burgdorferi, transmitted via tick bites. Untreated Lyme disease often leads to recurrent knee swelling, with about 60% of cases developing arthritis.
Most patients respond to a 30-day course of oral antibiotics like doxycycline or amoxicillin, while persistent cases may require intravenous antibiotics.
Hyperuricemia (Gout)
High uric acid levels, whether from genetics, metabolic syndrome, or reduced kidney excretion, can trigger gouty flares, including in the knee.
What are the Symptoms of a Swollen Knee?
The signs of a swollen knee can vary depending on the cause, but common symptoms include:
Visible swelling around the kneecap or general enlargement of the joint.
Tightness or stiffness, often with a feeling of fullness or pressure.
Pain, ranging from mild discomfort to severe throbbing, especially when bearing weight or moving the knee.
Warmth and redness if inflammation or infection is present.
Limited range of motion, making it difficult to fully bend or straighten the knee.
Instability or locking, particularly with mechanical injuries like ligament or meniscus tears.
Systemic symptoms such as fever, chills, or fatigue, in cases of infection or autoimmune disease.
Because swelling can hide underlying injuries or joint damage, any persistent or severe knee effusion should be evaluated by a healthcare professional.
What are the Common Risk Factors of a Swollen Knee?
Certain factors increase the likelihood of knee swelling. These include:
Age: Older adults are more susceptible to degenerative conditions, such as knee osteoarthritis.
Previous Knee Injuries: A history of fractures, ligament tears, or meniscal injuries predisposes to future swelling due to residual instability and cartilage damage.
Obesity: Excess body weight increases mechanical load on the knee, accelerating cartilage wear and predisposing to osteoarthritis.
Physical Activity: High‑impact sports or occupations that involve repetitive kneeling, squatting, or twisting increase injury risk. Conversely, insufficient physical activity weakens the muscles that support the knee.
Medical Conditions: Rheumatoid arthritis, gout, pseudogout, lupus, psoriasis, and metabolic diseases can cause recurrent joint inflammation.
Genetics: Family history of osteoarthritis or connective tissue disorders may increase susceptibility.
What are the Complications of a Swollen Knee?
Untreated or chronic knee effusion can lead to several complications:
Infection: Delayed diagnosis of septic arthritis allows bacteria to destroy cartilage and enter the bloodstream, potentially causing sepsis.
Chronic Pain and Disability: Persistent swelling from osteoarthritis or inflammatory arthritis results in ongoing pain, reduced mobility, and diminished quality of life.
Joint Instability: Ligament injuries that cause effusion may lead to ongoing instability and increased risk of recurrent injuries.
Reduced Range of Motion: Effusion and synovial thickening limit joint motion, leading to contractures.
Post‑Traumatic Osteoarthritis: Long‑standing swelling after trauma accelerates cartilage degeneration and can lead to secondary osteoarthritis.
Blood Clots (Deep Vein Thrombosis): Immobilization and inflammatory states increase the risk of venous thromboembolism.
How to Diagnose a Swollen Knee?
You can often tell a knee is swollen by comparing it to the other side: a swollen knee looks puffy or larger, the skin may appear shiny or stretched, and the joint can feel warm, tight, or painful, especially when you try to bend or straighten the leg.
You may also notice uneven contours, reduced motion, or a sense of pressure or fullness inside the joint.
Healthcare providers usually follow a stepwise approach to diagnose a swollen knee:
1. Clinical Evaluation
Diagnosing a swollen knee starts with a detailed history and physical exam:
History: Clinicians ask about the onset (sudden or gradual), prior injuries or infections, activity level, medications, comorbidities, and symptoms such as fever or rash.
Inspection & Palpation: The knee is checked for asymmetry, bruising, deformity, warmth, tenderness, effusion, and patellar mobility. Joint line tenderness is also assessed.
Range of Motion (ROM) & Special Tests: Active and passive ROM are compared to the other knee. Specific tests, such as the Lachman (ACL), posterior drawer (PCL), McMurray (meniscus), and patellar apprehension tests, help pinpoint injuries.
2. Imaging Studies
Imaging helps confirm diagnoses and assess structural damage:
X‑Ray: First‑line imaging to evaluate fractures, degenerative changes, and patellar alignment.
Ultrasound: Useful for detecting joint effusions, guiding aspirations, and evaluating bursitis or soft tissue injuries.
Magnetic Resonance Imaging (MRI): Gold standard for visualizing ligaments, menisci, cartilage, and bone marrow lesions. MRI can detect occult fractures, bone contusions, and synovial proliferation.
Computed Tomography (CT): Provides detailed bone images for complex fractures or preoperative planning.
3. Arthrocentesis (Joint Aspiration)
When the etiology is unclear or infection is suspected, joint aspiration is invaluable. Under sterile technique, a needle is inserted into the joint to withdraw fluid.
The fluid is analyzed for color, clarity, viscosity, white cell count, crystals, and microorganisms. This distinguishes inflammatory from non‑inflammatory effusions, identifies septic arthritis, and diagnoses gout or pseudogout.
Therapeutically, removing fluid can relieve pressure and improve mobility. Intra‑articular corticosteroid injection may be performed concurrently for inflammatory conditions.
4. Laboratory Tests
The following blood tests can aid in diagnosis:
Complete blood count (CBC) and C‑reactive protein (CRP)/Erythrocyte sedimentation rate (ESR)
Uric Acid Test
Rheumatoid Factor (RF) and Anti‑CCP
Antinuclear Antibody (ANA)
Culture and Gram Stain
Swollen Knee Treatment Options
Treatment for a swollen knee depends on the underlying cause, the severity and duration of symptoms, and other factors.
Mild or short-term swelling from minor injuries can often be managed at home. Still, persistent, recurrent, or severe swelling may require medical evaluation and targeted interventions, or surgical options may be considered to address the issue.
At home
For many minor injuries and mild inflammation, conservative management suffices:
Rest: Avoid activities that worsen pain; short periods of limited weight‑bearing and the use of crutches may be necessary.
Ice: Apply cold packs for 15–20 minutes every few hours during the first 48–72 hours to reduce swelling.
Compression: Elastic bandages or sleeves help limit swelling; ensure they are not too tight.
Elevation: Keeping the knee above heart level assists venous return and reduces edema.
Non‑steroidal Anti‑Inflammatory Drugs (NSAIDs): Ibuprofen or naproxen relieve pain and inflammation. However, caution is needed in patients with kidney disease or gastrointestinal ulcers.
Activity Modification and Bracing: Temporarily avoiding high‑impact activities and using a knee brace can stabilize the joint during healing.
Physical Therapy: A structured rehabilitation program restores range of motion, strengthens surrounding muscles, improves balance, and reduces the risk of recurrence.
Minimally Invasive Procedures
When conservative measures fail, minimally invasive interventions may be considered:
Corticosteroid Injections: Intra‑articular corticosteroids reduce inflammation and provide rapid symptom relief for conditions like rheumatoid arthritis, gout, or OA flares. However, repeated injections may damage cartilage or increase the risk of infection.
Platelet‑Rich Plasma (PRP) Injections: PRP, derived from the patient’s own blood, contains growth factors that may promote tissue healing. Emerging evidence suggests benefit in early osteoarthritis and chronic tendon injuries.
Hyaluronic Acid (Viscosupplementation): Injecting hyaluronic acid aims to improve joint lubrication in osteoarthritis. Some patients experience modest pain relief lasting several months.
Cryoablation: Freezing sensory nerves can provide longer‑lasting pain relief in chronic conditions. It may be considered in select patients after other therapies fail.
Surgical Management
Surgery is reserved for severe injuries or advanced disease:
Arthroscopic Surgery: Minimally invasive arthroscopy allows surgeons to repair or remove torn meniscal fragments, trim damaged cartilage, reconstruct ligaments (ACL or PCL), or remove loose bodies.
Open or Arthroscopic Fracture Fixation: Stabilizes displaced fractures to facilitate healing and early mobilization.
Synovectomy: Surgical removal of inflamed synovial tissue may be performed in refractory rheumatoid arthritis or pigmented villonodular synovitis.
Total Knee Replacement (Arthroplasty): Replaces the diseased joint surfaces with artificial implants. This procedure is considered when pain and swelling severely limit function and conservative treatments fail.
Postoperative Care and Rehabilitation
Following surgery, appropriate postoperative care is essential:
Pain Management: Multimodal analgesia (NSAIDs, acetaminophen, opioids, nerve blocks) and cryotherapy help control pain.
Early Mobilization: Guided by surgeons and physical therapists, patients begin gentle ROM exercises and weight‑bearing as tolerated to prevent stiffness and blood clots.
Physiotherapy: Progressive strengthening and endurance exercises restore function and reduce the risk of complications.
How to Prevent a Swollen Knee?
Although not all causes of knee swelling are preventable, adopting healthy habits reduces the risk:
Protective Equipment: Use knee pads during sports and occupations that involve frequent kneeling or contact.
Weight Management: Maintaining a healthy body weight reduces mechanical stress and lowers the risk of osteoarthritis.
Low‑Impact Exercise: Incorporate activities like swimming, cycling, or elliptical training that minimize joint stress while maintaining cardiovascular fitness.
Proper Technique: Learn proper form for sports and weight lifting to avoid sudden twisting or hyperextension injuries.
Stretching: Regular stretching of the quadriceps, hamstrings, and calf muscles maintains flexibility and reduces strain on the knee.
Early Management of Chronic Diseases: Prompt treatment of autoimmune diseases, metabolic syndrome, and gout reduces flare‑ups and joint damage.
Regular Monitoring: Individuals at high risk (athletes, older adults, and those with prior knee injuries) should undergo periodic medical evaluations to detect early changes.
Frequently Asked Questions (FAQs)
Can a swollen knee be dangerous?
Yes. While many causes are benign, rapid swelling accompanied by fever, severe pain, or inability to bear weight may signal a fracture, ligament tear, or septic arthritis and should prompt immediate medical attention. Delay in treatment increases the risk of permanent damage and systemic infection.
What can I do for a swollen knee at home?
Follow the RICE protocol: rest, ice, compression, and elevation. Use NSAIDs for pain if safe. Avoid activities that exacerbate symptoms. However, if swelling lasts more than a few days or recurs frequently, see a healthcare provider.
How long does it take for knee swelling to go down?
The time it takes for knee swelling to go down depends on the cause and severity of the injury or condition. Mild swelling from minor strains or overuse may improve within a few days to a week with rest, ice, compression, and elevation. Whereas swelling from more significant injuries, such as ligament tears, fractures, or hemarthrosis, can take several weeks to months to resolve, especially if rehabilitation or medical treatment is required. Chronic conditions such as arthritis or gout may cause intermittent swelling that persists or recurs over time and often requires ongoing management to control inflammation.
When should I worry about a swollen knee?
You should worry about a swollen knee if it is sudden, severe, or persistent, or comes with warning signs. Seek urgent care if you have rapid swelling, inability to bear weight, severe pain, deformity, redness, warmth, fever, or numbness. See a doctor soon if swelling doesn’t improve after a few days, recurs, causes locking or instability, or is accompanied by systemic symptoms. Early evaluation helps prevent joint damage and identify serious causes such as infection, fractures, or ligament injuries.
What happens if a swollen knee is left untreated?
Ignoring persistent swelling can lead to complications such as cartilage degeneration, chronic instability, decreased range of motion, and, in cases of infection, joint destruction and sepsis.
What does a swollen knee indicate?
A swollen knee indicates that there is excess fluid in or around the joint, which is usually a sign of an underlying problem rather than a condition on its own. It can result from injuries (ligament tears, meniscus tears, fractures), degenerative changes (osteoarthritis), infections (septic arthritis, bursitis), inflammatory or autoimmune diseases (rheumatoid arthritis, lupus), or crystal deposits (gout, pseudogout). The swelling reflects inflammation, bleeding, or fluid buildup in the knee, and its cause determines the severity, associated symptoms, and treatment required.
What does a swollen knee look like?
A swollen knee usually appears larger or puffier than the other knee. The skin may look shiny, stretched, or tight, and the joint can feel warm to the touch. Swelling may cause uneven contours around the kneecap or along the joint line. In some cases, redness or bruising is visible, and the knee may appear stiff or slightly deformed. Swelling can make it difficult to fully bend or straighten the leg.
Conclusion
A swollen knee is a symptom with many possible causes, ranging from traumatic injuries such as ACL or meniscus tears, fractures, and patellar dislocations, to inflammatory conditions such as rheumatoid arthritis, gout, and pseudogout, to degenerative osteoarthritis in older adults.
Serious infections like septic arthritis and bursitis require prompt recognition and treatment, while less common systemic causes include SLE, Lyme disease, and metabolic disorders.
Early diagnosis and intervention are crucial to prevent complications, reduce pain, and preserve joint function. Therefore, proper evaluation, including history, physical exam, imaging, and lab tests, helps identify the underlying cause and guide effective treatment.
Heavy periods that interfere with your daily life. Pelvic pressure that makes you uncomfortable. Frequent trips to the bathroom. If these symptoms sound familiar, you might be among the millions of women dealing with uterine fibroids.
At Seamless Medical Centers, we believe knowledge empowers better health decisions. Understanding what fibroids are and recognizing their symptoms is the first step toward reclaiming your comfort and confidence.
What Are Uterine Fibroids?
Uterine fibroids are noncancerous growths that develop in the smooth muscle cells of the uterus. These growths can appear alone or in groups and range dramatically in size, from as small as a grain of rice to as large as a melon. While the exact cause remains unclear, research indicates that genetics, age, race, and prolonged estrogen exposure may increase your risk.
The numbers tell a compelling story: An estimated 20% to 50% of women of reproductive age currently have fibroids, and up to 77% of women will develop fibroids sometime during their childbearing years. Despite their prevalence, many women suffer silently, accepting symptoms as “normal” parts of womanhood.
Recognizing Fibroid Symptoms
Fibroids don’t always cause symptoms, but when they do, the impact on your daily life can be significant. Common symptoms include:
Heavy and Prolonged Bleeding: Women with fibroids often have periods lasting longer than seven days that can be very heavy, requiring changing sanitary protection frequently.
Pelvic Pressure and Pain: Large fibroids can create a feeling of fullness in your lower abdomen or cause chronic pelvic discomfort.
Urinary Issues: Frequent urination or difficulty emptying your bladder completely when fibroids press against the bladder.
Digestive Problems: Constipation or rectal pressure when fibroids affect nearby organs.
Reproductive Challenges: In some cases, fibroids can contribute to fertility issues or pregnancy complications.
Types and Locations Matter
Understanding where your fibroids are located helps determine the best treatment approach. Our specialists classify fibroids by their position:
Subserosal: Located on the outer wall of the uterus, typically causing bulk or pressure symptoms.
Intramural: Within the muscular walls, often causing heavy bleeding or pressure.
Submucosal: Inside or near the uterine cavity, usually causing heavy bleeding and the least common type.
The size, location, and number of fibroids influence both your symptoms and treatment options.
Modern Treatment: Beyond Traditional Surgery
Gone are the days when hysterectomy was the only solution for problematic fibroids. Today’s minimally invasive approaches offer effective relief while preserving your uterus and dramatically reducing recovery time.
At Seamless Medical Centers, we specialize in advanced techniques that target fibroids precisely while protecting healthy tissue. Uterine Fibroid Embolization (UFE) is a new, FDA-cleared uterine sparing, outpatient procedure for uterine fibroids that utilizes recent technological advancements in instrumentation and imaging.
Your Path Forward
If fibroid symptoms are affecting your quality of life, you have options beyond “waiting it out” or accepting major surgery. Our team of board-certified interventional radiologists brings decades of experience in minimally invasive procedures that can restore your comfort and confidence.
We believe every woman deserves to live free from the limitations that fibroid symptoms can impose. During your consultation, we’ll review your medical history, discuss your symptoms, and create a personalized treatment plan that aligns with your goals and lifestyle.
Take the First Step
Ready to see if UFE is right for you? Contact Seamless Medical Centers to schedule your consultation. Our experienced team will evaluate your specific situation and help determine if PAE is the right choice for your specific needs. Most major insurance plans cover our procedures, and our team handles the authorization process for you.
Urinary incontinence (UI) means leaking urine when you don’t want to. It is a common health problem that affects millions of people, especially women and older adults.
Over 33 million Americans suffer from some type of urinary incontinence or bladder condition.
Although it becomes more common with age, it is not a normal part of getting older. UI usually happens because the bladder cannot store urine properly, or the muscles that hold urine in become weak.
Importantly, it can affect daily life. People may feel embarrassed, avoid social activities, or feel stressed. For caregivers and family, UI increases physical and emotional strain.
But do you know what makes this problem even harder?
There is a lot of stigma around urinary incontinence, which makes people think leaking urine is “normal” after childbirth or as they get older. This stops many from asking for help.
In this blog, we’ll break down everything you need to know about urinary incontinence, its types, causes, symptoms, risks, diagnosis, treatment, and prevention.
With the right information, people can get help sooner, and healthcare providers can offer better care.
What is Urinary Incontinence?
Urinary incontinence (UI) means losing control of your bladder and accidentally leaking urine.
This can happen in different ways: you might leak a little when you cough or sneeze, feel a sudden urge to pee, or, in rare cases, lose full control of your bladder.
Your urinary system includes several organs that work together to filter, store, and remove waste as urine. When everything is working normally, you can get to the bathroom on time.
Incontinence happens when these organs or muscles don’t function properly. There are many reasons this can occur, and it can affect people at any stage of life.
While it’s true that the risk increases with age, UI can affect anyone, young or old.
The good news is that treatments are available to help manage it. With the right care, incontinence doesn’t have to disrupt your life or stop you from staying active.
Types of Urinary Incontinence
There are several types of urinary incontinence, each with its own causes, symptoms, and triggers. Understanding which type you have is an important step in getting the right treatment.
The main types of incontinence include:
1. Stress Incontinence (SUI)
Stress incontinence (SUI) occurs when the pelvic floor muscles and/or urethral sphincter cannot resist sudden increases in intra‑abdominal pressure. Activities such as coughing, sneezing, laughing, exercising, or lifting heavy objects cause involuntary leakage.
In women, SUI commonly results from pregnancy, vaginal deliveries, and menopause, which weaken pelvic supports and the urethra. In men, it is frequently a postoperative complication of radical prostatectomy or transurethral resection of the prostate.
SUI is the most prevalent type in women; a cross‑sectional analysis of U.S. adults found that stress incontinence occurred in about 37.5% of women reporting incontinence.
2. Urge Incontinence (UUI)
Urge incontinence (UUI) is characterized by a sudden, intense urge to urinate followed by uncontrollable leakage. It is commonly associated with overactive bladder (OAB), a syndrome of urinary frequency, urgency, and nocturia.
Detrusor muscle overactivity is the principal mechanism; triggers include bladder inflammation or irritation (such as urinary tract infections), neurologic disorders (e.g., stroke, multiple sclerosis, Parkinson’s disease), and aging.
According to NHANES data, UUI affects approximately 9–31% of U.S. women and 2.6–21% of men, with prevalence rising sharply after age 75.
3. Mixed Incontinence (MUI)
Mixed incontinence (MUI) combines both stress and urgency symptoms. Research shows that 20–30% of individuals with chronic incontinence have MUI.
People may experience leakage with physical activity and a sudden urge to void. It is common in older women and is associated with the same risk factors as SUI and UUI.
4. Overflow Incontinence (OFI)
Overflow incontinence results from chronic urinary retention; the bladder becomes overdistended and leaks constantly or intermittently.
Causes include obstruction of urine outflow (e.g., enlarged prostate, urethral stricture), neurologic diseases causing impaired detrusor contractility (e.g., diabetic neuropathy, spinal cord injury), or medications that affect bladder emptying.
Also, overflow incontinence is potentially dangerous because it can lead to urinary tract infections and, in severe cases, kidney damage.
5. Functional Incontinence (FUI)
Functional incontinence arises when a person cannot reach the toilet or remove clothing in time.
Causes are external to the urinary tract, mobility impairments, cognitive disorders such as dementia, visual impairment, or environmental barriers.
While often overlooked, functional incontinence significantly contributes to incontinence in frail older adults and nursing home residents.
What Causes Urinary Incontinence?
Urinary Incontinence has multifactorial causes that can be temporary or persistent. Recognising the underlying cause is essential because treatment strategies vary.
Temporary Causes
Urinary Tract Infections (UTIs): Infections can irritate the bladder, leading to sudden urges to urinate and leakage.
Dietary Triggers: Foods and drinks like caffeine, alcohol, spicy foods, citrus fruits, carbonated drinks, and artificial sweeteners can irritate the bladder. Drinking large amounts of fluid or taking diuretics can also overwhelm the bladder.
Medications: Diuretics increase urine production, while some sedatives, muscle relaxants, or anticholinesterase drugs can interfere with bladder or sphincter control.
Constipation: Hard or impacted stool can put pressure on the bladder and block urine flow.
Acute Illnesses or Delirium: Confusion from illness or delirium can make it harder to recognize the need to use the bathroom or get there in time.
Persistent or Long-Term Causes
Key persistent and long-term causes include:
Pregnancy, Childbirth, and Menopause
Pregnancy and childbirth stretch and injure pelvic tissues and nerves. Vaginal delivery, instrument‑assisted birth, and having multiple births increase the risk of later SUI.
During menopause, declining estrogen causes atrophy of the urethral mucosa and pelvic connective tissue, reducing urethral closure pressure.
Aging
Age‑related changes include reduced bladder capacity, diminished urethral sphincter tone, and decreased estrogen in women.
Detrusor muscle overactivity becomes more frequent with aging. Evidence from the CDC’s Rise for Health study shows that women with multiple chronic conditions had poorer bladder health than those with zero or one chronic condition.
Overweight and Obesity
Excess body weight increases intra‑abdominal pressure and weakens pelvic floor muscles.
Another cross‑sectional study from NHANES 2013‑2018 reported that the weight‑adjusted waist index (WWI) was positively associated with urge urinary incontinence; each unit increase in WWI was associated with a 20% increase in UUI risk.
The study concluded that weight‑loss interventions could reduce UI in overweight women and clinically obese men.
Neurological Disorders
Stroke, spinal cord injury, Parkinson’s disease, multiple sclerosis (MS), and diabetic neuropathy can disrupt neural control of the bladder and urethra.
For example, MS and spinal cord injury can cause detrusor overactivity or detrusor-sphincter dyssynergia (outflow obstruction). Alzheimer’s disease and other dementias contribute to functional incontinence by impairing recognition of bladder signals or the ability to reach a toilet.
Pelvic Floor Disorders and Connective Tissue Weakness
Pelvic organ prolapse, such as cystocele or rectocele, can displace the bladder and urethra. Loss of connective tissue strength (e.g., collagen disorders) predisposes to SUI. In men, benign prostatic hyperplasia (BPH) and prostate cancer can cause obstruction and overflow or stress UI.
Diseases and Comorbidities
Diabetes, chronic obstructive pulmonary disease (COPD), chronic kidney disease, asthma, and cardiovascular disease contribute to UI risk. Obesity‑related metabolic syndrome amplifies risk through systemic inflammation and hormonal changes.
A study using NHANES data found that sarcopenia was independently associated with increased risk of mixed and stress UI among women aged ≥60 and that sarcopenic obesity with a metabolically unhealthy phenotype conferred the highest risk.
What are the Symptoms of Urinary Incontinence
The main symptom of urinary incontinence is leaking urine before reaching the bathroom or during activities. Leaks can be small or large, occasional or constant, and the exact symptoms often depend on the type of incontinence.
Common symptoms may include:
Leaking urine during activities like coughing, sneezing, laughing, exercising, bending, or sexual activity
Bedwetting (enuresis)
Sudden, strong urge to urinate followed by involuntary leakage
Frequent urination (more than 8 times a day), including waking at night (nocturia)
Feeling that the bladder is full or unable to completely empty
Weak urine stream or needing to strain to urinate
Continuous dribbling or leakage without warning
Difficulty reaching the toilet in time due to mobility or cognitive issues
Who Is More Likely to Develop Urinary Incontinence?
Women are roughly twice as likely as men to experience UI; hormonal changes, pregnancy, and childbirth account for much of this difference.
Moreover, age is a strong predictor; prevalence increases from 3.7% among people aged 65–69 to 10.6% among those aged ≥85.
Race/ethnicity and socioeconomic status also influence risk; African American women have higher rates of urge or mixed UI, while white women are more likely to report stress UI.
Also, higher body‑mass index, diabetes, COPD, hypertension, and neurological disorders increase risk. Similarly, a study shows that sarcopenia, sarcopenic obesity, and metabolic unhealthy obesity were shown to elevate the risk of stress and mixed UI markedly.
In addition, research also highlights that environmental exposures to endocrine‑disrupting chemicals (e.g., bisphenol A) may specifically raise the risk of urge UI.
What are the Complications of Urinary Incontinence?
Urinary Tract Infections (UTIs): Incomplete emptying and catheter use increase the risk of UTIs.
Reduced Quality of Life: People may restrict social interactions and physical activities to avoid accidents, leading to isolation, depression, and anxiety.
Falls and Fractures: Rushing to the toilet increases the risk of falls, particularly among older adults.
Sleep Disruption: Nocturnal urgency and voiding disturb sleep, causing fatigue and cognitive impairment.
Caregiver Burden and Institutionalization: UI is a major reason for admission to long‑term care, and study shows that more than 50% of nursing home residents and 75% of long‑term care residents have UI.
Kidney Damage: Chronic urinary retention in overflow incontinence can lead to hydronephrosis and renal failure.
How Is Urinary Incontinence Diagnosed?
A thorough evaluation is essential to determine the type and cause of UI. Here’s how:
History & Physical Examination
The Doctor asks about when and how often leaks happen, fluid intake, medications, and health history. They check your abdomen/pelvis and may do a “cough stress test” to see if leakage happens with pressure.
Bladder Diary
You record when you drink, when you pee, how much, and when leaks occur (for several days). This helps identify patterns and triggers.
Urinalysis & (if needed) Urine Culture
A urinalysis checks for urinary tract infection (UTI), blood, sugar, or other abnormalities that might explain incontinence. Also, blood tests are sometimes performed to evaluate kidney function or detect other systemic conditions. These blood tests assess renal function, glucose, calcium, and electrolytes.
Post-Void Residual Measurement
After you urinate, a test (via ultrasound or catheter) may measure how much urine remains in your bladder. If a large amount remains, this may indicate incomplete bladder emptying (overflow or neurogenic bladder).
Bladder Function (Urodynamic) Tests
For more complex or unclear cases, tests such as uroflowmetry, cystometry, or pressure-flow studies assess how well your bladder and sphincter store and release urine.
Cystoscopy or Imaging
If there’s suspicion, endoscopic or radiographic evaluation is performed to assess for abnormalities, bladder stones, tumors, or fistulas.
Urinary Incontinence Treatment Options
Treatment should be individualized based on the type of incontinence, severity, age, sex, and comorbidities.
Management usually follows a stepwise approach: lifestyle modifications, behavioral therapies, medications, devices, and surgery.
Lifestyle Changes
These are first‑line strategies recommended for all patients because they have minimal side effects and address reversible factors.
A frontiers study of 20,195 adults found that adherence to 4–5 healthy lifestyle factors (non‑smoking, moderate alcohol intake, regular physical activity, healthy diet, and optimal waist circumference) reduced the risk of overactive bladder by 46% compared with adherence to 0–1 factors.
Here are some lifestyle and behavioral therapies to consider:
Pelvic Floor Muscle Training (PFMT)
Also called Kegel exercises, PFMT strengthens the levator ani and urethral sphincter. People contract and relax pelvic muscles in sets of 10–15 squeezes, three times daily.
Evidence indicates that PFMT improves or resolves symptoms in two-thirds of women. Men benefit as well; PFMT is recommended after prostate surgery.
Lifestyle Modifications
Maintain a healthy weight, treat chronic cough, manage diabetes and constipation, stop smoking, reduce alcohol and caffeine intake, and avoid bladder irritants.
Fluid Management
Drink adequate fluids (about 6–8 glasses daily) and avoid excessive intake. Avoid drinking right before bedtime.
Behavioral Therapies
Behavioral therapies help retrain the brain–bladder connection and reduce anxiety, urgency, and leakage through mental and emotional techniques.
Bladder Training and Timed Voiding
For urgency or mixed incontinence, patients gradually increase intervals between voids and use urge‑suppression techniques. This helps expand bladder capacity and reduce urgency.
Cognitive Behavioral Therapy (CBT)
CBT helps individuals modify thoughts and behaviors that exacerbate urgency or fear of leaking. It teaches coping strategies, reduces bathroom-related anxiety, and improves confidence in bladder control.
Physical Therapies
Physical therapy focuses on strengthening and retraining the pelvic floor muscles to improve bladder control and reduce leakage.
Pelvic Floor Muscle Rehabilitation
This involves learning to strengthen and control the pelvic floor muscles, as they support the bladder and help prevent urinary leakage.
A physical therapist teaches proper techniques (similar to Kegel exercises). Therapy may also include breathing techniques and core strengthening to improve overall pelvic stability.
Biofeedback and Electrical Stimulation
Biofeedback uses sensors to display muscle activity on a screen, helping you learn when you’re contracting the right muscles and how to improve control.
Whereas electrical stimulation delivers a gentle current to activate weak pelvic floor muscles, strengthen them over time, and reduce symptoms like urgency, frequency, and leakage.
Together, they help improve muscle awareness, coordination, and bladder control.
Medications
Medication is usually considered when behavioral therapies don’t provide enough relief.
Common drug options include:
Anticholinergics (Antimuscarinics)
Antimuscarinic agents (e.g., oxybutynin, tolterodine, solifenacin) are used to relax the bladder muscle to reduce urgency, frequency, and urge-related leakage.
In U.S. Medicare data, antimuscarinics remain the most commonly prescribed, but their use decreased from 49% to 34% between 2012 and 2021, while β‑3 agonist use increased from 0.2% to 17%.
Beta-3 Agonists
These drugs (e.g., mirabegron, vibegron) also relax the bladder muscle but typically have fewer cognitive side effects than anticholinergics.
Topical Estrogen
Low-dose vaginal estrogen can improve urethral and vaginal tissue health, reduce irritation, and improve stress or urgency symptoms in postmenopausal women.
It is not the same as systemic hormone therapy and has minimal systemic absorption.
Medications for Men with BPH-Related Incontinence
For men with bladder symptoms caused by prostate enlargement, alpha-blockers (e.g., tamsulosin, terazosin) help relax the prostate and bladder neck. Whereas 5-alpha reductase inhibitors (e.g., finasteride, dutasteride) shrink the prostate over time. Often, these medications are combined for better symptom control.
Minimally Invasive Procedures
These treatments are considered when lifestyle changes and medications aren’t enough and offer effective, low-risk options to improve bladder control.
Botox Injections for Overactive Bladder
Botox is injected into the bladder muscle to calm overactive contractions. This reduces urgency, frequency, and the risk of sudden leakage. Results typically last 6–12 months.
A small device sends gentle electrical pulses to the sacral nerves, which control bladder function. This helps restore normal signaling and reduces urge incontinence and urinary retention.
Urethral Bulking Agents
A gel-like material is injected around the urethra to facilitate closure. This provides extra support and reduces stress incontinence, especially in women with weak sphincter muscles.
Surgical Treatments
These procedures are considered when other treatments fail or when incontinence is severe and linked to structural problems.
Mid‑urethral Sling Procedures
A mesh or tissue sling is placed under the urethra to provide support. It helps maintain urethral closure during coughing, laughing, or exercise, making it highly effective for stress urinary incontinence in women.
Artificial Urinary Sphincter (AUS) Implantation
AUS is most commonly used in men, especially after prostate surgery. It involves placing an inflatable cuff around the urethra, which opens and closes via a small pump. This provides strong control for moderate to severe incontinence.
Bladder Neck Suspension
This surgery lifts and secures the bladder neck and urethra into a better position. It helps reduce leakage caused by weak support tissues and is often used for stress incontinence in women.
Cystoplasty (Bladder Augmentation)
This procedure enlarges the bladder using a piece of bowel. It increases bladder capacity and reduces pressure, making it useful for severe urge incontinence or neurogenic bladder when other treatments have failed.
How to Prevent Urinary Incontinence?
You can lower your risk of urinary incontinence by protecting your pelvic floor and managing lifestyle factors: Here’s how:
Maintain a Healthy Weight: Keeping your BMI in a healthy range reduces pressure on your bladder. Weight-loss programs are especially effective for overweight women and obese men.
Avoid Bladder Irritants: Cut back on caffeine, alcohol, carbonated drinks, artificial sweeteners, spicy foods, and citrus. Some people also react to chocolate and acidic foods.
Stay Hydrated: Drink enough water to keep urine light-colored, but don’t overdrink. Dehydration can irritate the bladder and increase the risk of UTIs.
Prevent Constipation: Eat more fiber, drink plenty of fluids, and stay active. Constipation can worsen bladder leakage.
Do Pelvic Floor Exercises: Practice PFMT regularly, including during and after pregnancy, to keep pelvic muscles strong.
Quit Smoking: Smoking causes chronic coughing, which strains pelvic muscles and increases SUI risk.
Manage Chronic Conditions: Keep conditions like diabetes, hypertension, asthma, and COPD under control to protect bladder function.
Stay Physically Active: Regular exercise supports weight control and muscle strength. Avoid too many high-impact activities if they trigger leakage; balance them with PFMT.
Frequently Asked Questions (FAQs)
Can urinary incontinence be cured?
Many people achieve significant symptom improvement or complete resolution, especially with early intervention. Lifestyle and behavioral therapies (PFMT, bladder training) are effective first‑line treatments. For persistent symptoms, medications, neuromodulation, or surgery can provide relief. Cure rates vary by type and severity; for example, research shows that PFMT cures or improves symptoms in roughly 67% of women, while mid‑urethral sling surgery for SUI has long‑term success rates around 80%. Urge incontinence often requires combination therapy; Botox and sacral neuromodulation have similar efficacy at two years.
Is urinary incontinence a normal part of aging?
No. Although prevalence increases with age, UI is a medical condition, not an inevitable consequence of aging. Many older adults maintain continence with proper bladder health habits, pelvic floor exercises, and management of chronic diseases.
Will drinking less water help with incontinence?
Restricting fluid intake can worsen urinary symptoms because concentrated urine irritates the bladder. Instead, spread fluid intake throughout the day and limit fluids before bedtime. Avoid caffeinated or carbonated beverages, as they can’t stimulate the bladder.
When should I see a healthcare provider about incontinence?
You should consult a clinician if you experience involuntary leakage that affects daily life; have associated symptoms such as burning, pain, blood in urine, or frequent UTIs; or have difficulty emptying your bladder. Early evaluation helps identify reversible causes and prevents complications.
Conclusion
For many people, talking about bathroom habits can feel embarrassing. However, it is a common and often overlooked condition that affects millions of Americans.
Urinary incontinence may make you self-conscious or keep you from enjoying daily activities because you’re worried about leaking or not reaching the bathroom in time.
Therefore, promoting bladder health, encouraging early symptom reporting, and supporting lifestyle changes are essential.
Most individuals can achieve meaningful improvement through weight management, pelvic floor exercises, bladder training, and appropriate medications or procedures.
If you’re experiencing any signs of incontinence, don’t wait; taking action now can help you prevent discomfort and bigger problems later in life.